------------------------------------------
Heat illnesses, flu outbreak in the military, a new mRNA flu vaccine, and more
The Dose (June 30)
Somehow it’s already July. And with it comes the heat, along with the health consequences that follow. We’re also seeing a rise in the virus behind many sore throats, plus some possible early Covid-19 signals in the South.
A military flu outbreak continues to increase after the removal of a vaccine requirement. A summer flu outbreak? Yes, it’s possible, and yes, it sure feels like we’re spending an awful lot of energy undoing lessons earlier generations learned the hard way, only to reinstate them once we've relearned why they existed.
We’ll close with some good news and a question from the YLE community: Does DEET attract mosquitoes?
Here’s what’s going on, and, most importantly, what it means for you.
Disease weather report
Heat risk rises
Large swaths of the U.S. will be dangerously hot this week, on the heels of an extreme heat wave in France that led to 1,000 excess deaths across 5 days. The risk in the U.S. peaks Thursday, when more than 170 million people will be in areas at “high” or “extreme” health risk from heat.
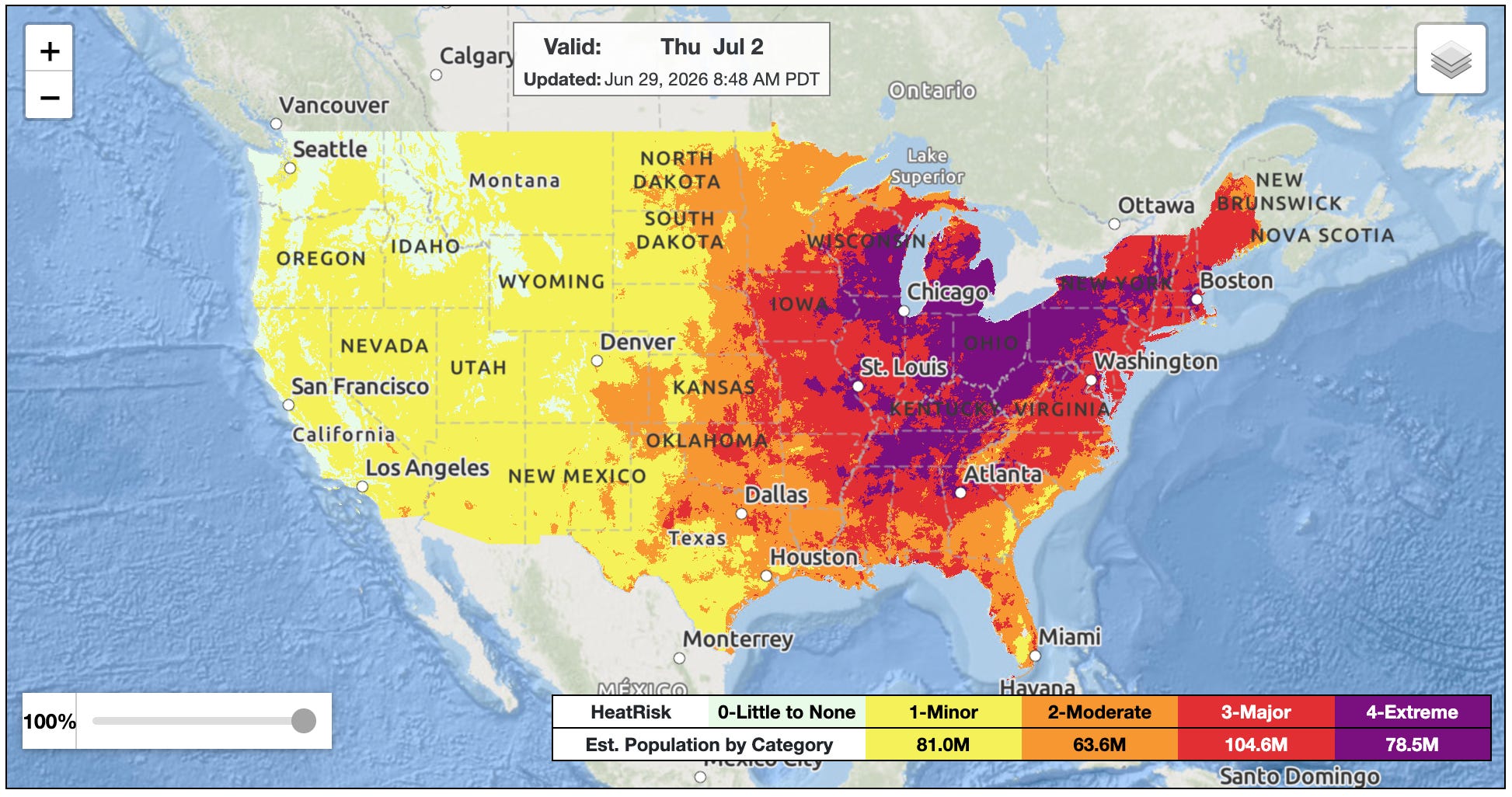
What this means for you: If you live in the red or purple patches above, everyone needs to take action, not just those who are high-risk. Enter your zip code for guidance. YLE will be back tomorrow with more tips and tricks.
Very small signs of Covid-19?
Every summer, the U.S. sees a Covid-19 wave, and this year should be no different, though the big question is how large it will get. Each year’s summer wave has been smaller than the last, and I hope it eventually becomes a blip.
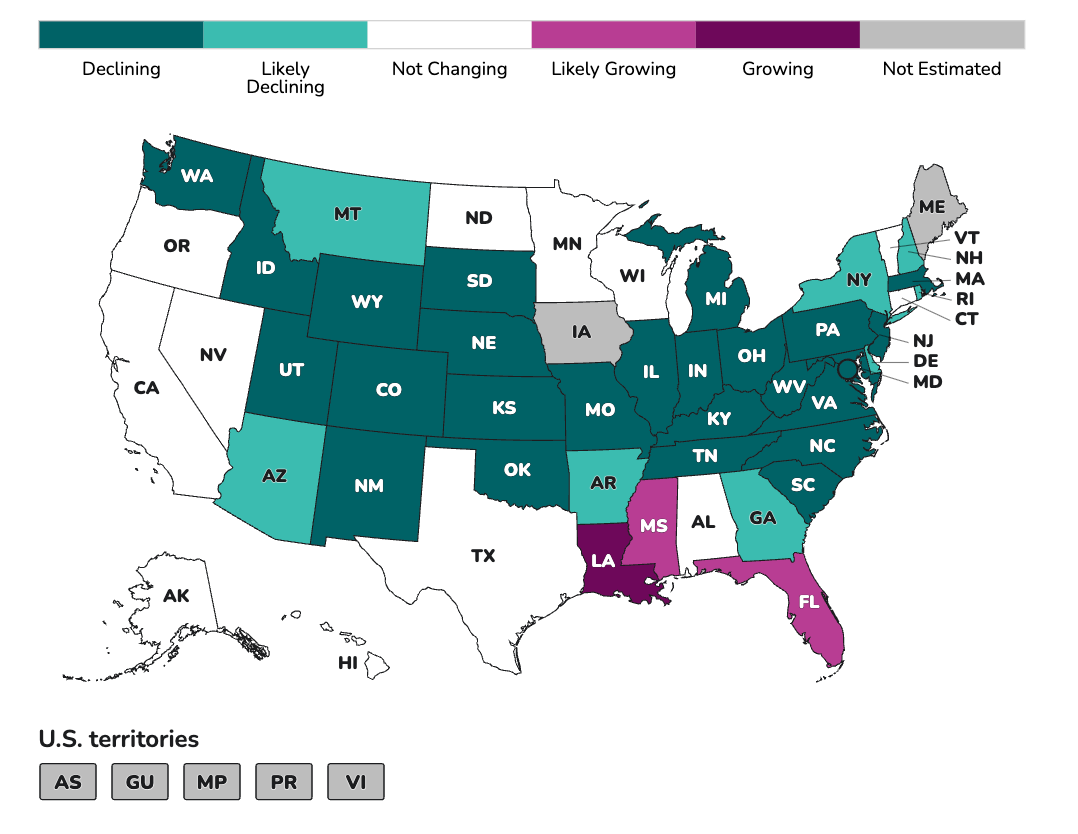
Nationally, wastewater levels are extremely low, among the lowest we’ve seen in a very long time. But movement is starting in Southern states, and emergency department visits there, while still low, are beginning to climb. This is typically where the summer waves begin.
Healthy Cup
We’re in week 3 of the World Cup, and no major outbreaks are tied to the games other than heat-related illnesses.
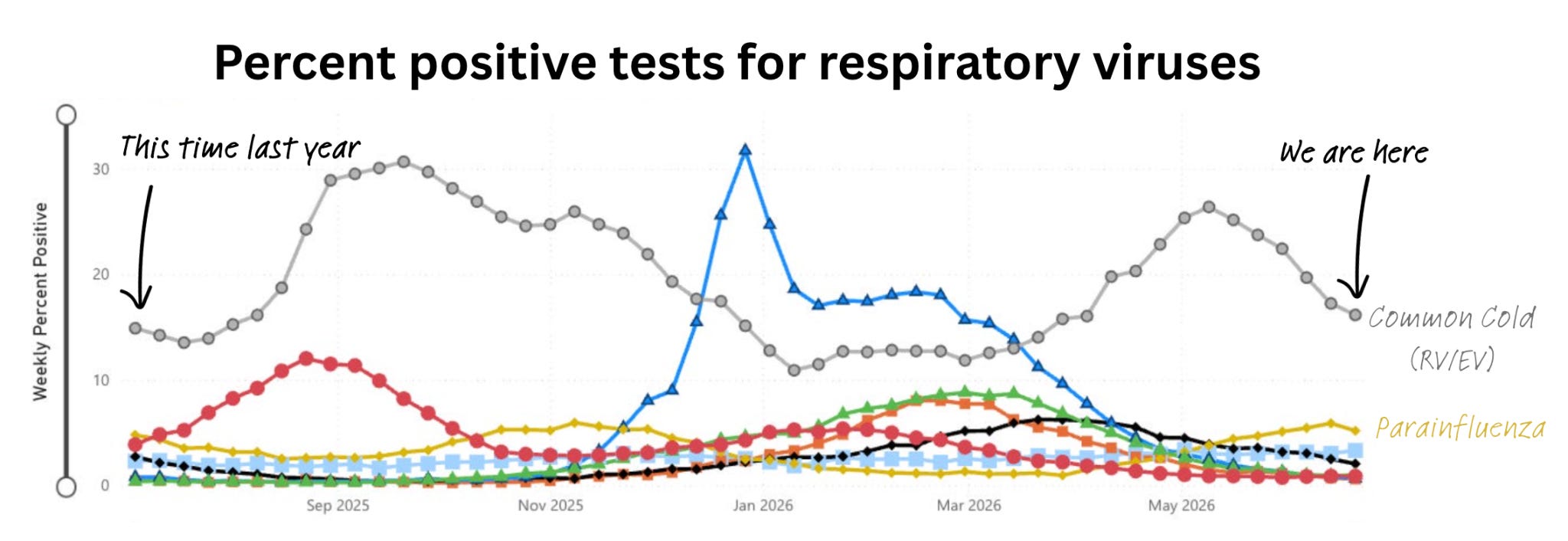
The YLE team detected increased chatter on social media about unidentified cold-like illnesses, including reports of a sharp sore throat, body aches, cough, headache, and fever. Some viruses do peak at this time of year, such as parainfluenza. (See the yellow line below.)
When the Health Security Operations Center looked into it using a more advanced wastewater technique, another virus—called parechovirus—also showed a rapid increase. This doesn’t have a common test in clinical or wastewater settings, so it usually flies under the radar. Most people catch this virus in childhood, and it is spread through close contact. It’s often mild, with few or no symptoms, though it can cause cold-like symptoms. It’s most severe for infants, where it can rarely cause meningitis.
What this means for you: If you’re feeling crappy, it may be one of these viruses, and the normal tests at a doctor’s office will come up negative. For most healthy people, both are mild and clear up on their own. Rest and drink plenty of fluids. And, as always, call your physician with questions.
—Julia Tellerman, YLE epidemiologist at the Health Security Operations Center.
Spotlight: Military flu outbreak follows a vaccine requirement policy change
You’ll notice the flu didn’t appear in the disease weather report above. Yet a flu outbreak has hit the military just weeks after a policy change made vaccination optional for active-duty service members. Nearly 300 at a boot camp are now sick.
How is a flu outbreak during summer possible? And is it truly because of the policy change?
What is unfolding at these training camps is essentially a combination of bad luck after a risky policy:
Flu never disappears. A big June outbreak is unusual, but flu doesn't vanish in summer; it just drops to very low levels. Wastewater for Flu A is essentially zero right now, with only sporadic Flu B. But a spark is possible.
Once it sparks, the environment plays a big role. And this is a unique environment. Spread comes down to a few things: environment (human behavior), weather (cold, dry air), and the usual unknowns. Recruits live, eat, sleep, and train in tight quarters around the clock, so even with summer weather working against it, the virus has room to move. Epidemiologists have watched flu burn through summer-camp dorms for exactly this reason. Wider community spread is unlikely, though: the weather is wrong, school is out (students are a major driver of transmission), and recruits confined to base have little outside contact.
Policy impacts behavior. The general public doesn’t get vaccinated this time of year, since there’s generally not much flu to vaccinate against. But basic training is the exception: according to veterans, recruits are vaccinated on arrival, regardless of the month. After the requirement was dropped, only about 40% of new recruits chose the shot, down from near-universal coverage before (roughly 99% in the Navy, Air Force, and Marines, and about 98% in the Army). We don’t know whether this outbreak was caused by the same flu strains the vaccine covers.
Dropping the flu vaccination requirements is a scientifically and economically risky decision. The requirement had been in place since the 1950s for one simple reason: military readiness depends on keeping troops healthy and in the field. Remember, the Spanish flu took as many American lives in the barracks as battle did in WWI.
So, did this outbreak dent readiness? This is important because it’s one of the rationales for a requirement. This is where a denominator would help, and I haven’t found one reported publicly. Three hundred sick out of 400 means basically the whole base went down, which is bad for preparedness. The same 300 out of 6,000 is under 3%, which seems more manageable.
The vaccine requirement was quietly reinstated last week. This is the right call, as this outbreak foreshadows the possibility of an outbreak affecting all troops during the actual flu season. That certainly would impact military readiness.
As epidemiologists say: Bugs have ears.
Good news
Medicare gets access to reduced-price GLP-1s. Starting Wednesday, some Medicare recipients will be able to get the drugs for a $50-a-month co-payment. Here are the criteria. The coverage is only for a temporary trial period, set to expire at the end of 2027.
Naloxone options expand. The FDA approved another over-the-counter nasal naloxone. More options on the shelf mean more competition, lower prices, and easier access to a medication that can reverse an opioid overdose in minutes. Wider availability saves lives.
A new mRNA flu vaccine. Remember that flu vaccine that RFK Jr.’s FDA said they wouldn’t review and then, after immense backlash, reviewed again? Well, we got exciting news: the external FDA advisory panel voted 9-0 to back Moderna’s mFlusiva (mRNA-1010), set to be the first mRNA-based seasonal flu vaccine in the U.S. In a trial of over 40,000 adults aged 50 and older, it cut symptomatic flu by about 27% compared with a standard shot, with a bigger effect on hospitalizations and immune responses than even the high-dose senior vaccine. With a final FDA decision expected by August 5, it could be available for the 2026–2027 season.
But there’s a major wrinkle. The U.S. has no functioning ACIP, due to ongoing legal battles between the American Academy of Pediatrics and RFK Jr. So while the FDA may call it safe and effective, no one is in place to set policy on who gets it and when. That likely means Americans won’t have access to this vaccine this fall, but it’s worth following closely.
Question grab bag
Any truth to the study that DEET might attract mosquitoes?
There is no evidence DEET intrinsically attracts mosquitoes. A recent 2026 lab study showed that they can be conditioned to associate fading DEET with food, prompting many headlines. This associative learning from mosquitoes is fascinating, but the number of times a mosquito feeds over its natural lifespan is in the single digits (3-5ish, depending on species). There has also been some research suggesting that a single mosquito species may become somewhat desensitized to it over time.
The practical takeaway remains the same, though: keep using DEET and reapply regularly. It remains one of the most effective preventive measures we have against mosquitoes, and we are enterinig mosquito-borne illness season.
—Dr. Marisa Donnelly, YLE NY correspondent, trained in mosquito-borne illnesses.
Bottom line
Heat is the immediate health threat this week, so start there (check your zip code). But the bigger takeaway is that the public’s health suffers when systems quietly stop doing the boring things that keep us safe.
Love, YLE
Your Local Epidemiologist (YLE) comprises a team of experts, ranging from physicians to immunologists to epidemiologists to nutritionists, working together with one goal: to “translate” ever-evolving public health science so that people are well-equipped to make evidence-based decisions. The YLE suite of newsletters reaches over 475,000 people across more than 132 countries.













.jpg)
No comments:
Post a Comment