-------------------------
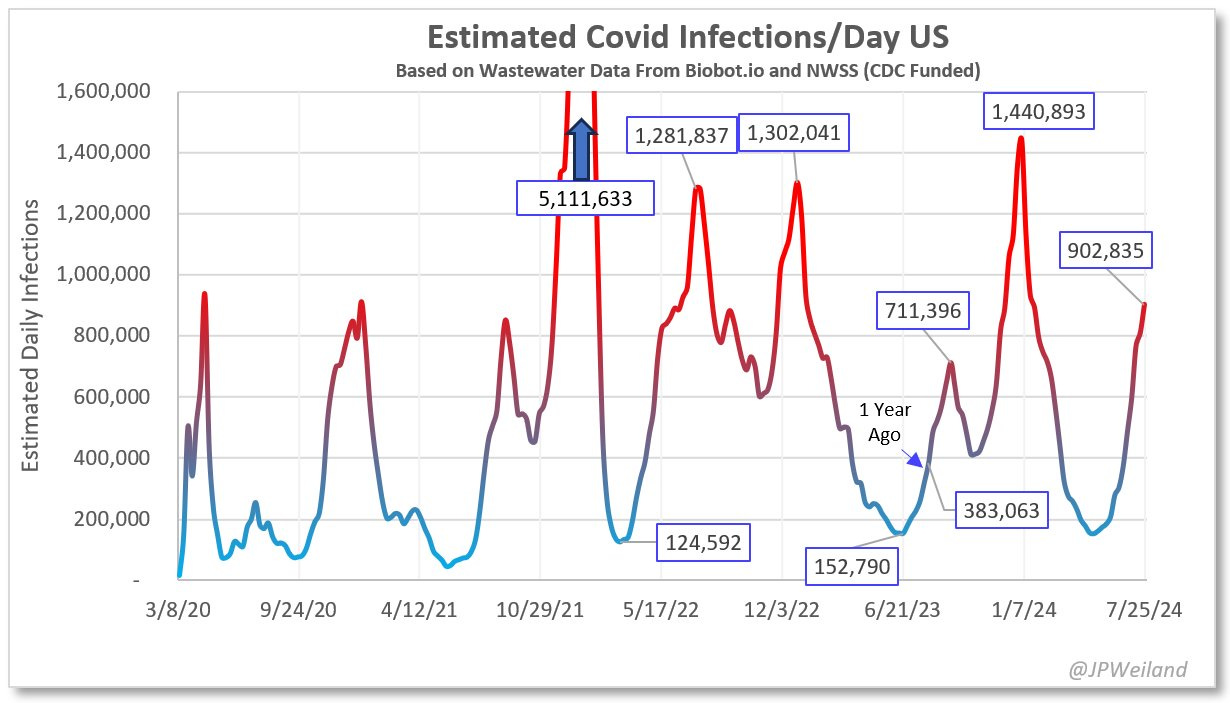
It’s a major wave now, with an estimated new 900,000 infections per day, as my friend Jay Weiland estimated based on the 2 sources of US wastewater data (definitely worth following him at X or Threads). The slope of rise of SARS-CoV-2 levels is still steep, so we haven’t yet reached the plateau. It’s already towered beyond 4 prior waves of the US pandemic.
State-of-the-Wave
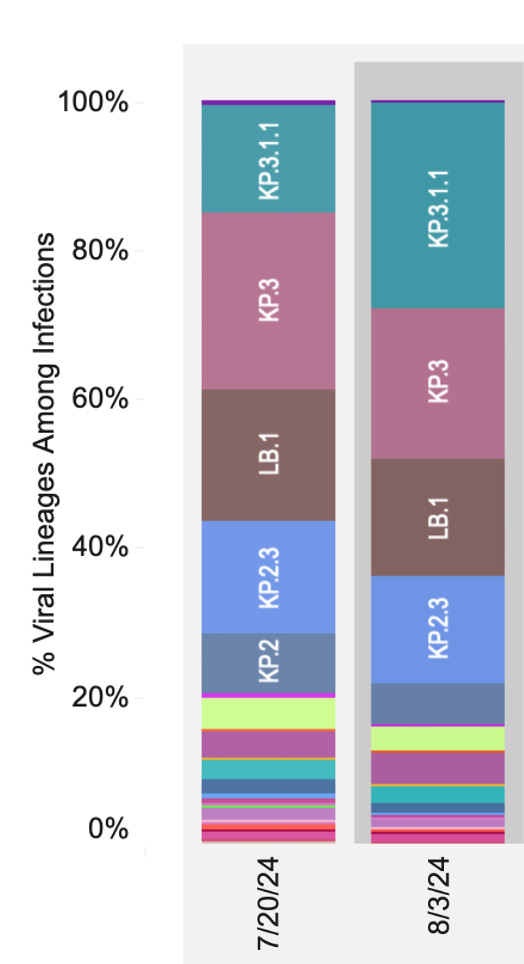
It’s related to the variants KP.3 and KP.3.1.1, which together now account for more than half of new cases in the US. And KP.3.1.1 is on the move, overtaking KP.3 as shown by the new CDC data below. A big jump in the past 2 weeks.
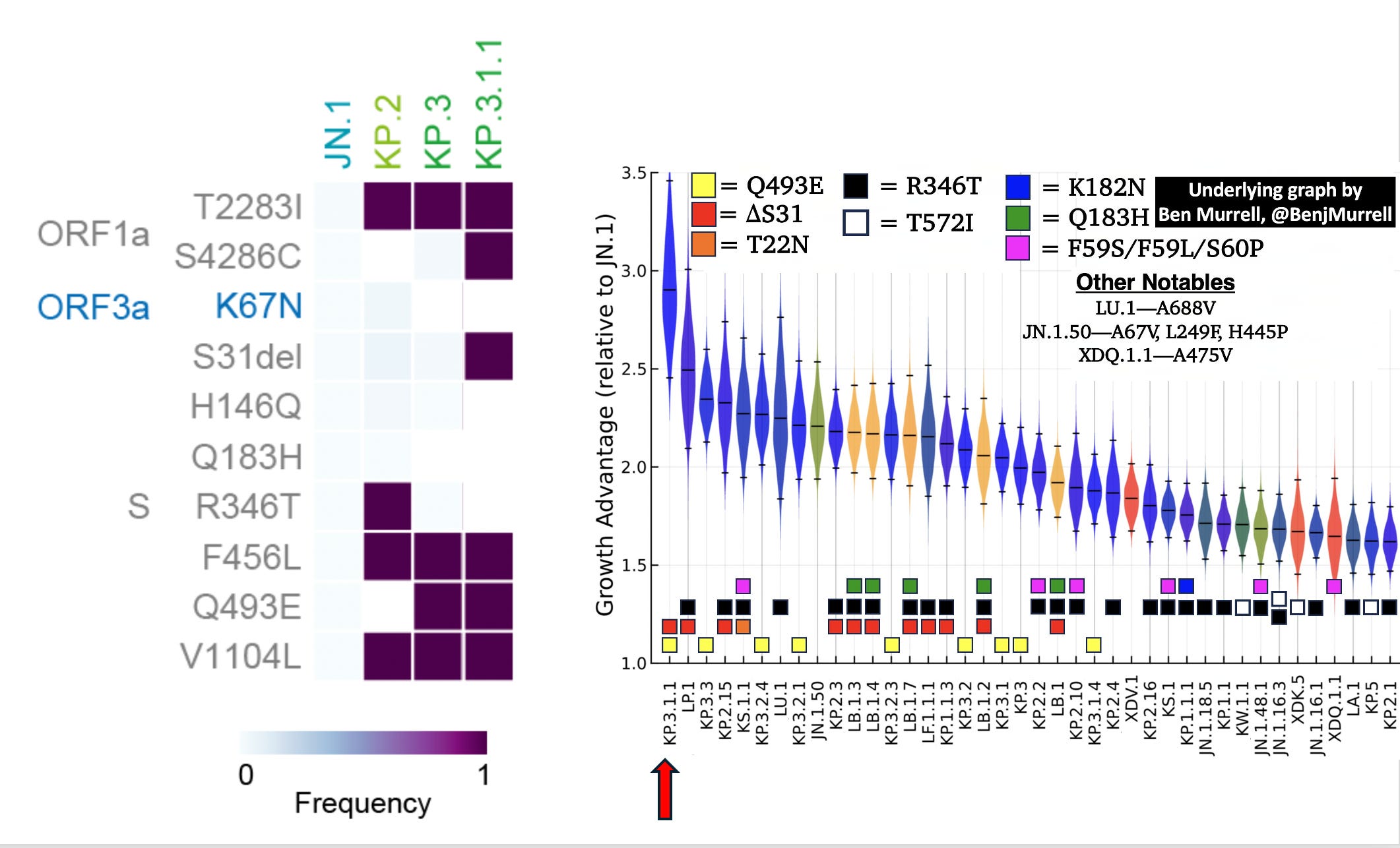
We’ve known about the decided growth advantage of the KP.3 and KP.3.1.1 variants for many months. Back in April I wrote here about the concerns over a new wave indexed to these FLiRT variants derived from JN.1 that hit us hard last winter. The FLiRT acronym comes from the new mutations F456L and R346T that showed up in KP.2, as seen at left below. (S-spike, ORF-open reading frame). But note below, it’s no longer FLiRT, since KP.3 does not have the R346T mutation. Instead there’s the Q493E mutation in KP.3 and, added to that, the S31 deletion in KP.3.1.1. The Sato Lab in Japan recently characterized KP.3.1.1, as having the most immune evasion and infectivity of any of the variants derived from and including JN.1. And previously Ben Murrell showed clearly (below, right) KP.3.1.1 had the most prominent growth advantage of all circulating variants out there. No surprise it is rapidly rising to dominance here and elsewhere around the world.
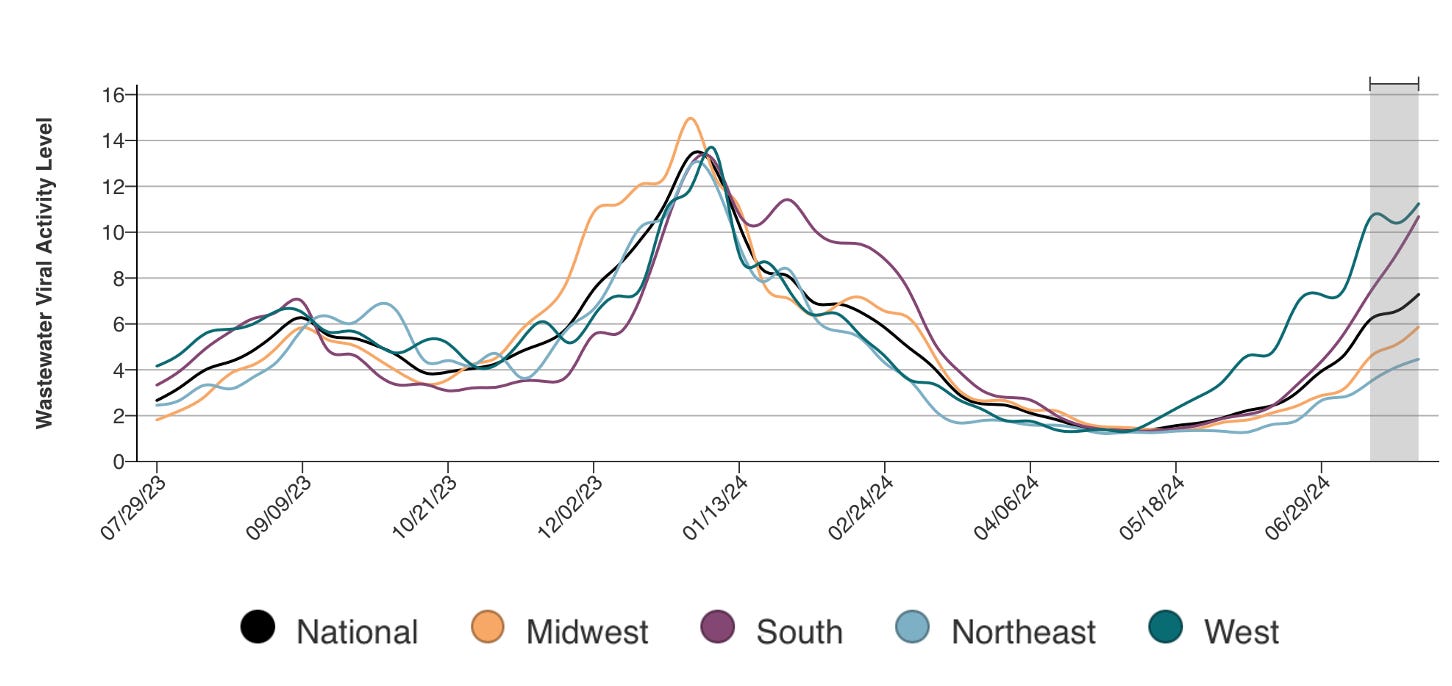
Fortunately, the rise in levels of the virus, still going up in all 4 major US regions (most recent CDC data below) has not been linked with as much severe Covid (absolute increase) as was seen in prior waves, but compared to last week there was a relative increase of 25% of deaths and 12% increase in emergency room visits due to Covid. No matter how you look at it, this is not a benign wave, folks.
Moreover, besides people getting sick from Covid, typically now from a recurrent bout (often 3rd or more), there will be more people developing Long Covid, as Ziyad Al-Aly and colleagues recently published—less new cases of Long Covid but still a risk, especially in unvaccinated individuals.
Why is this happening?
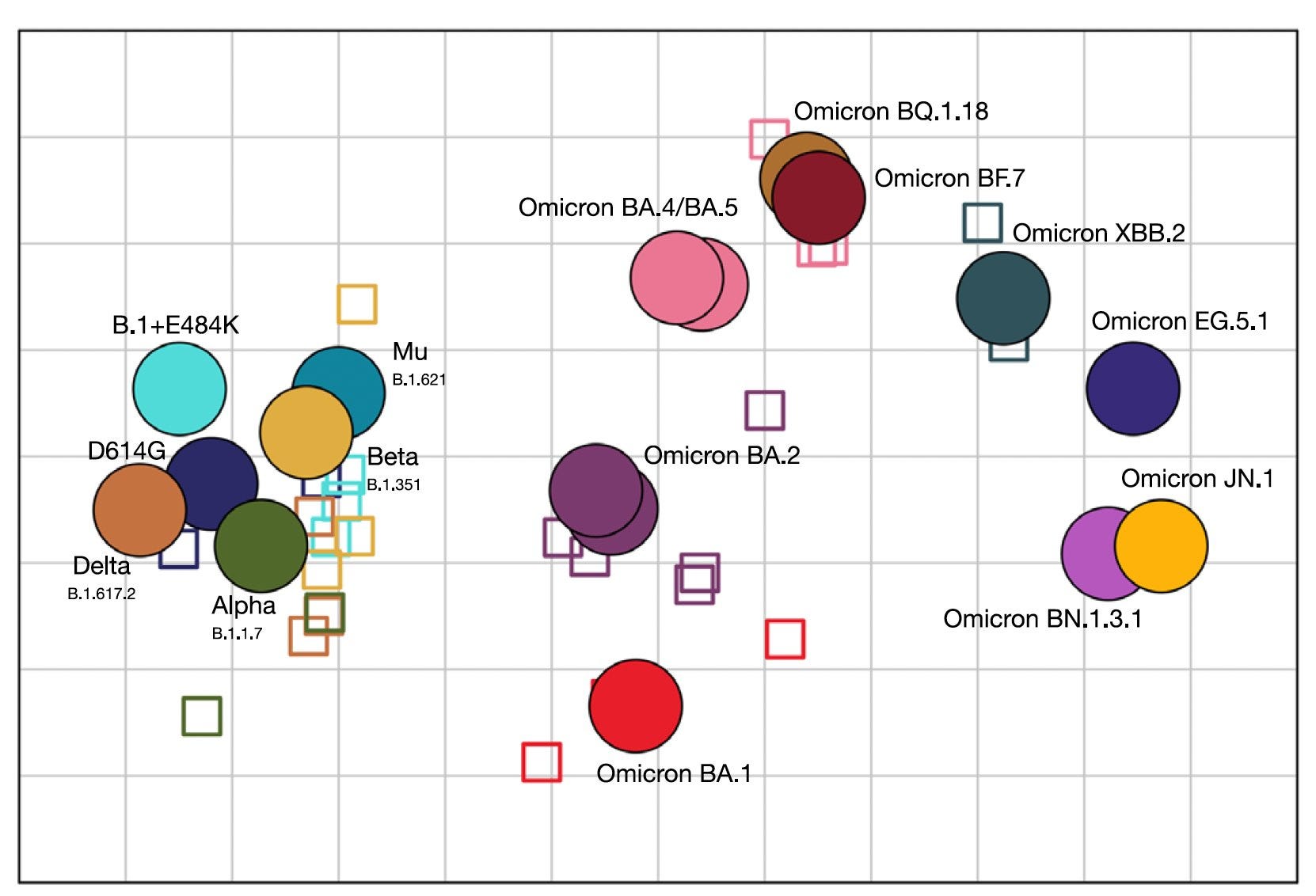
The virus is relentlessly evolving, getting further and further away as an antigen (how our immune system “sees” the virus) than the strains of virus in the early years of the pandemic. The antigenic distance map below reflects that evolution. JN.1 is further way from the infamous Omicron BA.1 than BA.1 is from the major variants of 2020 and 2021 (Wuhan-ancestral, D614G, Alpha, Delta, Beta). KP.3 and KP.3.1.1. is to the right of JN.1 (not shown), even further away. The virus will not stop here, despite our desire to will it way. It will continue to find new ways to infect and reinfect us, under selection pressure from our prior immunity (be it infections, vaccinations, or combinations). We may also see another “Omicron-like event” in the times ahead, with a profoundly altered virus spike, tens of new mutations, as seen with BA.1 and BA.2.86 (the latter eventually led to JN.1)
Added to problem of the virus‘s evolution and, as a result, is the blunting of our immune response, the big issue of waning immunity. The vaccine boosters only last 4-6 months for protection from severe Covid, do little after early weeks for any protection from infections or spread. The same goes for infections. Neutralizing antibody levels go down. Our interferon first line of defense gets blocked (Shane Crotty called this the “superpower of SARS-CoV-2” in our podcast this week). The virus evolves and, at the same time, our immune response wanes. That’s not a good combination.
The other feature that promotes the virus is our complete let down of mitigation that we know (despite misinformation and disinformation) works. Few people are masking. Little has been done to improve air quality or ventilation. Indoor events are being held with big crowds, making believe that the virus has gone away. It hasn’t. It won’t.
What Can We Do About It?
Covid is not like Flu for an annual shot
For convenience, and opposed to all the data, the FDA has tried to force fit Covid to be like Flu and that’s wrong. It doesn’t take a genius to see we have 2 major waves each year and, for high-risk individuals, semiannual (every 6 months) shots will be needed for protection. And those shots have to be aligned with the strain of the virus.
We knew about KP.3 lurking in March but didn’t have the FDA Advisory Committee meeting until June, at which time it was decided the KP.2 booster vaccine (Pfizer, Moderna) would be the way to go, and JN.1 for Novavax. That meeting should have taken place in April, at the latest, and a new booster would have been available in about 90 days. This is all happening because of the wrong read on Covid being like seasonal flu.
What about right now?
The new KP.2 boosters will not be ready until the first week of September. It isn’t clear about the timing of availability for the JN.1 shots from Novavax which the company announced at the June FDA meeting would be ready in August. Most likely all 3 will be rolled out the first week of September. The match up of KP.2 (vs KP.3.1.1) than JN.1, but some people prefer Novavax with its less acute phase side effects.
That’s still more than month away. The XBB.1.5 (old) booster is available and it will increase protection, so if you’re worried about making a trip or being exposed, it’s a reasonable strategy to get it. While suboptimal, the added level of protection afforded from that booster is useful.
Of course, it’s never just about vaccines. We are all cognizant of the various mitigation factors that help protection (if only we used them).
Longer Term Strategy
Nasal Vaccines
We have to get nasal vaccines into high gear to markedly reduce infections and spread. This week I did a Ground Truths podcast with Shane Crotty, one of the leading US immunologist and virologists, on his landmark paper in Nature. By doing nasal and nasopharyngeal swabs every month in 100 participants throughout a year of the pandemic, his team identified the determinants of nasal (mucosal) immunity, which we aren’t going to get from shots. He, like me and many others, including Akiko Iwasaki, remain quite optimistic we’ll get a successful nasal vaccine. That was reinforced by a report from the Washington University group that developed a nasal vaccine and licensed it to India (where it is approved and used). In hamsters, a widely used and accepted experimental SARS-CoV-2model, their nasal vaccine blocked spread. Besides blocking transmission, it reduced infectious virus titers ~100-fold and 100,000-fold in the upper and lower respiratory tract, respectively, of the primary contact following SARS-CoV-2 exposure. That did not occur with mRNA shots.
The investment of the US for Project NextGen has been minimal to develop nasal vaccines with only 2 programs supported and it’s moving quite slowly. I don’t understand why the Washington University nasal vaccine is not being assessed in the US, including regulatory guidance and oversight. And there are many other candidates from academic labs at Mt. Sinai, Emory ,Yale and others. What a missed opportunity.
More Durable, Universal (Pancoronavirus) Covid Vaccines
Our vaccines have sat in stagnation since the miracle of their appearance and potency in late 2020. No change in nanoparticles to enhance the acute immune response or make it more durable. No willingness to get a self-amplifying vaccine here that uses far less mRNA, and already approved in Japan. Academic labs have identified more than 50 templates for a pan-betacoronavirus or pan-sarbecovirus vaccine but most of this work sits in high-tier peer review publications, not being used to get a variant-free vaccine tested. It’ll ultimately take longer than a nasal vaccine but we’re essentially in standstill mode with little investment in moving forward. Hwo shortsighted this is. The funds available through Project NextGen certainly are inadequate to get this effort supported. The variants will keep coming and we’ll just keep chasing them, being months behind. We can and must do better than this!
Our best defense against Long Covid is not to get Covid. Our second best known defense is to be vaccinated. The better the vaccine, the less Long Covid risk.
Treatments for Long Covid
Well over a billion US dollars that have been wasted (RECOVER) without clinical trials of very promising candidate drugs. Yesterday Bernie Sanders proposed a new moonshot fund of $1 billion per year for 10 years for dedicated Long Covid research.. That’s terrific but there are 2 problems. For one, it is highly unlikely to actually get funded, and we’ll have to wait until next year to see if a new Administration and Congress will be supportive. Until now, even the words “Long Covid” have not been uttered by the current President, no less definitive action to get treatments assessed. With millions of Americans suffering Long Covid, it would be politically wise to acknowledge this public health crisis and get all over it. Second, we have already seen how poorly the NIH did in deploying cumulatively about $1.5 billion for this purpose (and nothing to show for it), so I don’’t see how pouring more funds into a failed experiment makes sense. We need the funds and new efficient models for expeditiously testing repurposed or new drugs in large, rigorous clinical trials. With all we’ve learned about the pathophysiology, nicely reviewed this week by Trisha Greenhalgh and colleagues, we have the blueprints to run with this.
Thanks for reading and subscribing to Ground Truths.
Please share it!
You can subscribe to Ground Truths yourself at this link.













.jpg)
No comments:
Post a Comment