Out of control COVID means permanent segregation for many disabled people
It’s August, and we are once again in the throes of a major COVID wave.
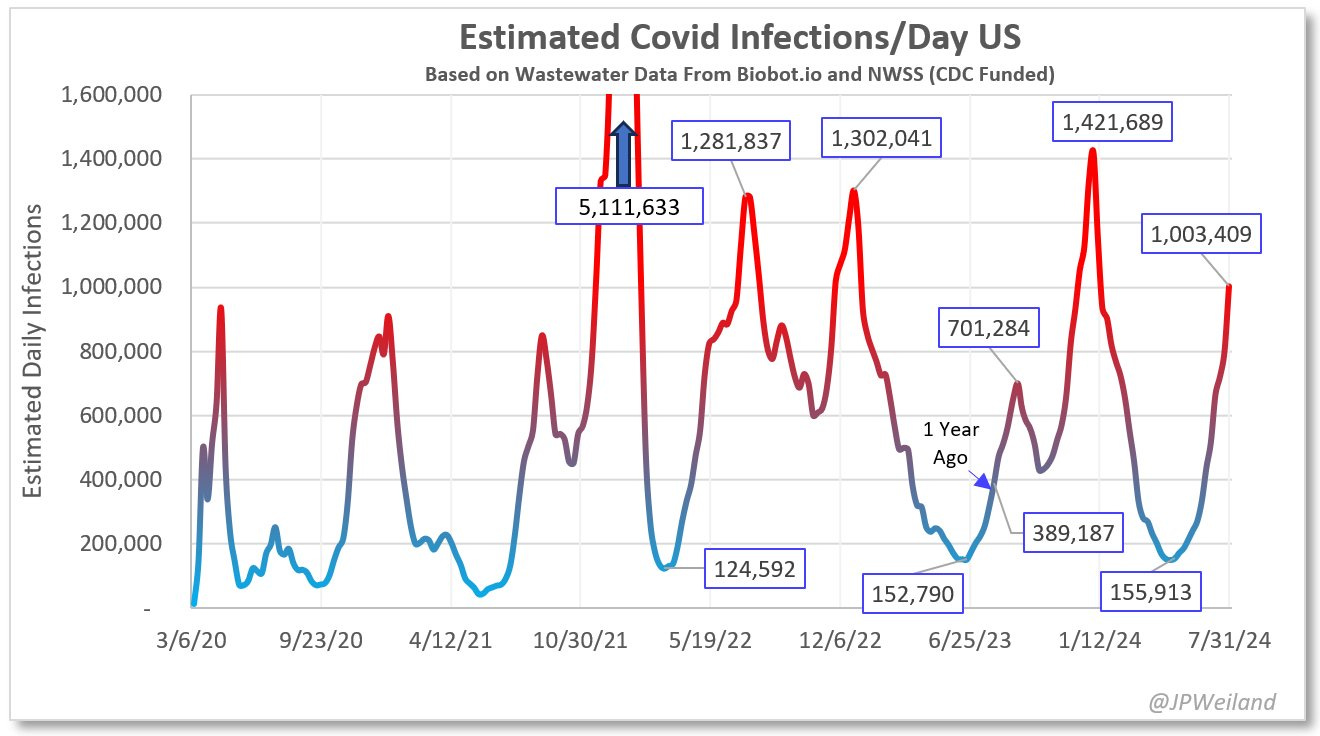
Using wastewater data- the only data that measures the amount of circulating COVID-19 in an era of inaccessible tests and discouraged reporting- infectious disease modeler J.P. Weiland estimates that the US has yet again crossed the million-infections-per-day mark as of August 9, with about 1 in 33 Americans currently infected with COVID-19.
The CDC, indeed, reports that over half of states have now crossed their “very high” threshold, and the raw wastewater data shows a dramatic upward swing.
1 in 33 means COVID in every restaurant, every supermarket, onboard every airplane, and of course in every hospital- where infection control teams continue to harm and kill vulnerable patients by failing to implement airborne infection control measures.
I’ve written before about how, in November 2021, nearly a year after the debut of the vaccines, Fauci publicly declared that US COVID cases would need to fall “well below 10,000 a day” for us to get a “degree of normality,” and allow us to return to pre-pandemic life. In the nearly three years since, the US has never had a single day with under 10,000 new COVID cases per day; in fact, we have never had a single day with under 100,000 new COVID cases per day.
Instead, in August 2024, we have over one million new COVID cases per day.
Is over a million new COVID cases per day “well below” 10,000 new COVID cases per day? Or did this administration pivot and sell a public health failure as a public health victory?
When we talk about the failures of the vaccine-only approach to COVID, it’s important to understand what the goals of that approach were. Why did Fauci believe we would have under 10,000 cases a day, and why was that important?
Fauci and other officials around the world hoped and believed that we would achieve herd immunity to COVID, if not through vaccination alone, then through a combination of vaccination and infections. Herd immunity would protect the vulnerable- including people who cannot themselves be vaccinated or who do not mount an immune response to vaccines- from COVID exposure.
It’s also important to keep disease transmission low because, frankly, diseases are not neutral events, even for nominally healthy and abled people. It’s not healthy to be reinfected with SARS-COV-2, or any virus, once or twice each year. Disease is economically costly due to worker absences and productivity slowdowns. “Healthy” and “abled” are also permeable categories; when you infect people with diseases more often, you increase the number of “unhealthy” and “disabled” people. By keeping transmission of SARS-COV-2 “well below” 10,000 cases a day, the community at large is returned to a state of pre-pandemic well-being.
This promised land of low transmission, clearly, never happened. To understand why, you can read my piece about viral evolution and vaccine evasiveness, which explores in depth how SARS-COV-2 evolved faster than expected and escapes immunity from both vaccines and infection within months (if not weeks). This immune evasiveness successfully got the virus to the other side of the failed vaccine-only strategy, and that’s where it’s really been able to stretch its legs. Because on the other side of the vaccine-only strategy, there is no plan B. There are no masks, no mitigations; there’s no plan, and no plan to make a plan.
Instead, the approach is one of denial, misinformation, hiding data, stripping resources, privatizing vaccines and medications, and turning those who (believe they) can play “back to normal” against those who simply cannot. “Herd immunity” has been redefined to mean … well, what exactly does it mean, in the context of the entire population being reinfected over, and over, and over again? To pundits it’s a shorthand for “most people have already had COVID before.” To politicians it’s an applause line equivalent to “COVID is over.” To the public, it just means, “I don’t have to care anymore.”
For immunocompromised people, disabled people, and other people avoiding COVID, it’s meaningless. Herd immunity to measles means vulnerable people are never exposed to measles. Herd immunity to SARS-COV-2 means vulnerable people are exposed every time they leave home.
It is not debatable, it is data: if 1/33 Americans currently have COVID, disabled and vulnerable people are being exposed to a disease that could kill or further disable them each time they leave home. And those COVID troughs between the giant, twice-yearly spikes aren’t a pass for disabled folks to breathe easy; the low point of this year’s brief lull was 155,913 new cases per day, or about 1/200 people concurrently infected. Surely, much better than 1/33. But hardly low. You won’t be boarding a commercial flight without risking COVID.
It’s important to stress that no other circulating virus spreads in this way, with this rate of reinfection; SARS-COV-2 isn’t the flu, it’s more severe, with more complex health implications. But even if SARS-COV-2 were a flu, flu doesn’t reinfect within months and circulate year-round. Current wastewater shows flu levels nationally at the lowest ‘minimal’ level. While we were previously assured that COVID would somehow “become seasonal,” now minimizers like Ashish Jha have pivoted to rhetoric like “typical summer wave”.
Seasonal influenza is nowhere near as contagious as SARS-COV-2, with reproductive numbers that vary between 1-2, with the linked research article at BMC Infectious Diseases finding that across 24 studies, the median estimated R0 of the deadly 1918 flu was 1.8. The R0 of SARS-COV-2 was estimated at 3.32 way back in 2020, and each new variant has carried warnings of increased transmissibility. A recent case study published in the American Journal of Infection Control found that an asymptomatic COVID+ patient infected a subsequent patient who was seen in the same examining room a full 4.5 hours later.
There have always been viruses, and there have always been immunocompromised people, but prior to COVID there was never this level of viral spread, with a virus of this severity, with this ability to reinfect, with this level of transmissibility. Immunocompromised people are under constant siege, with levels of disease unseen in modern times being normalized in all public spaces.
For many disabled and immunocompromised people, segregation is as complete as their need to avoid COVID. Indoor dining, of course, is out. Going to bars, happy hours, work events, weddings, conferences, parties, anything where large groups of people gather is a risk, even in a high-quality mask which will leave you unable to eat, drink, and a likely target for snide remarks and mocking jokes. Because again, the political messaging coming from the top encourages healthy people not only not to protect vulnerable people, but to mock and deride them.
If your political messaging is that COVID is “over” and “no big deal,” what are you communicating about those who still wear masks? That they are wrong, misinformed, ignorant, afraid, crazy, weak, strange, or stupid?
People who must work with the public often face a stark choice between protecting their health and protecting their career and/or income; those who feel they can risk another infection, and even many who can’t, are pressured to unmask in workplace settings and threatened with professional consequences or fired if they won’t. Others, including myself, have withdrawn from their careers entirely, finding no space for “a disabled person who still acknowledges the existence of COVID” in the conservative field of [checks notes] progressive campaign work.
Because the political messaging around COVID has been so violent and has hinged so explicitly on turning people who feel they can go “back to normal” on those who can’t, I now dislike attending gatherings as the only one in a mask. I know I am shadowed by years of propagandist language about my “fear”; I know that when others remain unmasked in the face of my assertion that I am at risk from COVID, they are choosing to believe political propaganda over my direct communication about my failing health. In this way this messaging has segregated us not just physically, but emotionally, cutting us off from both physical safety and our support systems.
And while large social events are risky and uncomfortable, professional excommunication for the crime of not being able to afford infinite COVID infections has left me utterly disillusioned with the progressive politicians I once worked for. When it comes to the disease that has already taken much of my functional capacity, silence is golden.
I am a good case study of a disabled person trying to navigate COVID, precisely because I did so much to avoid it and have still been harmed, and precisely because I do not “look sick.” Therefore, seeing me in a mask is particularly triggering to people who are so sure that COVID is a cold now.
I am invisibly disabled with several underlying health conditions, including hEDS (a connective tissue disorder) and POTS. For some time, it’s been known that hEDS increases your risk of Long COVID; this ongoing research reaffirmed my commitment to avoiding COVID. I rebuilt my life around trying to avoid infection, knowing that my baseline energy was already quite low; I turned down jobs that would have required office presence, left campaigning, moved into a one-bedroom apartment. I had to completely give up all indoor socializing in public, because indoor public spaces are unsafe for people like me.
Yet last November, I caught COVID for the first time from a houseguest. I tested him on the first day of his visit; he developed symptoms on his third. It is very difficult to avoid COVID when all of society is dedicated to maximizing, rather than minimizing, its spread. All the more so when “progressives” in my own extended circle can be as ignorant and as likely to infect as conservatives.
Despite taking Paxlovid and Metformin, I indeed went on to develop Long COVID, experiencing worsening of my underlying conditions as well as the development of new symptoms including chronic migraine.
Prior to last November, I was disabled but was doing low-impact workouts 4-5 days a week, holding a full-time job, and keeping up with my commitments while also managing to take a couple of vacations with friends. Since then, I can no longer workout, nor even go on long walks. I have trouble sitting up for long periods of time, and I have not left my house except for doctor’s appointments and MRIs since June 22, the day before my birthday. I cannot drink alcohol anymore or drive long distances. I haven’t been able to travel or go on a trip. I cannot hold a full-time job, and I currently devote most of my time to resting. This week I was told that I have two hip labral tears, one on each side, that no one can explain as I have barely moved in nine months but was experiencing worsening hip pain.
Essentially, a single COVID infection took me from functional to housebound with new onset, debilitating symptoms and strange injuries. I went from never having a headache to having round-the-clock migraines that don’t respond to OTC meds, for which I now take multiple expensive medications. What would a second COVID infection do to me?
Do I not deserve access to public spaces?
Do other disabled people not deserve access to public spaces?
Do I not deserve to live a life that is free from the constant threat of reinfection with a virus that already took so much from me? Do I have the right to socialize, to eat in a restaurant? After all, isn’t that what the people who refuse to mask claim? That a life without eating indoors is a life that isn’t worth living?
What about the millions of people who were disabled by their first, second or third COVID infections? Do they deserve to risk reinfection each time they leave home?
So much political messaging is dedicated to obfuscating the inconvenient reality that we exist- we, people who cannot afford another SARS-COV-2 infection, who indeed exist in our millions- because unending, unmitigated COVID is only justifiable in a world where unending, unmitigated COVID is no big deal.
Minimizing messaging has focused very heavily on conveying to the public that COVID is not harmful- even though nothing in the scientific literature supports this claim.
The “back to normal” facade can only function as long as “healthy” people believe that SARS-COV-2 infection is harmless; in order to maintain this illusion, people who have been or will be harmed by COVID must be thrown under the bus, and be labeled crazy, fringe, or even violent terrorists.
In other words, in the fight between COVID and disabled people, healthy/abled people cannot be neutral but must be oriented against either COVID or disabled people. The state knows this and moves aggressively to encourage the public to defend the right of COVID to exist in public spaces over vulnerable people. And they do.
Instead of holding the state accountable for what is a world-historical failure to control disease, instead of demanding a new approach to begin mitigating these unprecedented levels of public illness, the public is distracted with mocking, marginalizing, criminalizing, and attacking disabled people. Who, to be clear, are already completely excised from most forms of public life.
By minimizing COVID and thus encouraging abled people to maximize its spread, our politicians and media redirect the violent unresolved anger of the pandemic crisis at those most harmed; the disabled, and in particular those with Long COVID.
People who sincerely, in all other struggles for equity and justice, consider themselves on the side of the oppressed, are here aligned with the forces of the state advocating for maximum spread of COVID. And I do mean “maximum.” Because while the state continues to boast of a “toolbox” full of “tools”, a robust pandemic response with a properly educated and resourced public would see usage of those tools during a massive COVID surge.
Instead, most people are committed to doing nothing; not even masking indoors when not eating or drinking; not masking on airplanes; not testing before gathering; not advocating for new clean air standards or airborne infection control in healthcare; not anything. I would describe it as not so much passively doing nothing, but actively, violently doing nothing. Knowing they could mask, understanding how helpful it would be, and refusing out of spite, fear, anger, and again, the unresolved trauma of the pandemic crisis; all of it redirected at the few people who continue to try and call attention to the ongoing crisis.
The reason disabled people continue to be segregated from public life and isolated at home is that abled people refuse to acknowledge that they are. Because if it were acknowledged that millions of people are permanently locked out of society, that would shatter the illusion of the “normal” that never actually came back.
People who fight for health equity would have to do something.
People who value community would have to do something.
People who characterize themselves as caring and thoughtful would have to do something.
Progressives would have to do something.
The Democratic Party would have to do something.
The government would have to do something. And that is why governments around the world continue to tell the majority, the complacent public, the abled, the not-yet-disabled or not-yet-aware that ongoing, never-ending, unprecedented waves of disease in your communities is simply the new normal, and nothing can be done, and you do you, and learn to live with it.
This week the DNC will take place in Chicago. During a massive COVID wave where 1 in 33 are infected, they will not require masks nor negative COVID tests, and instead gather tens of thousands of people indoors, infecting thousands of them. 10% of those infected will go on to have new long-term health problems. And then that 10% will have to choose; continue playing back to normal and risk their remaining health, or join those of us by the wayside in an effort to protect what health they have left.
At this point I genuinely do not expect that I will ever be able to eat in a restaurant or drink in a bar again; I don’t particularly think about it anymore. I am more concerned about COVID exposures on flights to see loved ones and particularly, in needed upcoming surgeries in medical settings. What is more painful than not being able to rejoin the world is the lack of anger from those who cosplay 2019 without us. The back to normal fantasy isn’t harmless, though its victims are always just out of sight. It’s a machine running on bodies; our eyes, ears, stomachs, brains, hearts, immune systems, livers, and kidneys. If you don’t stop feeding the machine, eventually it will be your body too.
There is no neutrality in this fight; if you don’t stand up for disabled people’s right to public spaces, you are advocating for COVID’s unchallenged right to reign over them all.













.jpg)
No comments:
Post a Comment