I've always known that the Republicans have a better sense of humor than the Democrats, who are too busy being offended to laugh. Since Trump's appearance at McDonald's, we've been having lots of fun at the Dems' expense.
COVID-19 is no longer the world’s leading infectious disease killer
"COVID-19 is still very much the topic of conversation when it comes
to infectious diseases, but when it comes to lethality, the coronavirus
no longer leads the pack.
"Instead, it’s tuberculosis
that has once again become the world’s most deadly infectious disease. A
World Health Organization report this week shows 10.8 million people
became sick with TB last year (with 8.2 million people being newly
diagnosed). Roughly 1.25 million of those people died because of the
disease.
"COVID deaths, meanwhile, have been significantly reduced thanks to
vaccines and treatments, though it still claimed 320,000 lives last
year.
“The
fact that TB still kills and sickens so many people is an outrage, when
we have the tools to prevent it, detect it and treat it,” WHO
Director-General Dr. Tedros Adhanom Ghebreyesus said in a statement.
“WHO urges all countries to make good on the concrete commitments they
have made to expand the use of those tools, and to end TB.”
"The number of new infections last year was the highest since the WHO began monitoring TB in 1995.
"Tuberculosis largely affects people in 30 countries. More than half
the global cases are found in India (26%), Indonesia (10%), China
(6.8%), the Philippines (6.8%) and Pakistan (6.3%).
"COVID, ironically, is partially responsible for the rise in TB cases.
Disruptions from that virus hampered TB services across the globe,
letting it increase. There’s also a strain of TB that has proven resistant to several drugs.
Global funding for TB prevention has also decreased and funding for TB
research only reached 20% of its target amount in 2022, the WHO said.
"Tuberculosis is a contagious bacterial infection of the lungs that is normally spread through the air. Most tuberculosis infections are asymptomatic and
not contagious. Active tuberculosis, however, which is characterized by
cough, fever, decreased appetite and weight loss, can be very
contagious and dangerous disease if left untreated, sometimes resulting
in death."
"As we approach a new presidency, a new Congress and new leaders in
our health agencies, I am concerned that the sense of urgency about
COVID-19 appears to have faded. The disease has not been discussed
during the election season, even though it is an ongoing and developing
public health threat.
"I believe this is a dangerous mindset. The reality is that COVID-19
remains a unique and deadly threat for many people — it is not just
another respiratory virus, and should not be treated as such by our
leaders.
"I am the CEO and co-founder of biopharmaceutical InflaRx. But I am
also an intensive care physician and researcher active in the immunology
field. I have worked in the ICU. The reality is clear: We may be done
with COVID-19, but COVID-19 is not done with us.
"The virus continues to cause fatalities, even outside of the
traditional respiratory season. During the summer of 2024, the Centers
for Disease Control and Prevention reported
that COVID-19 killed thousands, with about 4,200 reported deaths in
August alone. As of October, some 40,000 Americans have lost their lives
to COVID-19 in 2024.
"A study published in the Journal of the American Medical Association
in May 2024 found that in the fall and winter of 2023-2024, the risk of
death in patients hospitalized with COVID-19 was greater than the risk
of death in patients hospitalized for seasonal influenza. On Sept. 28,
2024, the CDC reported that COVID-19 hospitalizations continued to outpace flu and RSV hospitalizations combined.
"Despite these facts, the CDC website now groups COVID-19 with flu and RSV, stating that
“while COVID-19 still poses a significant threat to people at higher
risk, its health impact is now similar to other respiratory viruses,
like flu, which are also important causes of illness and death,
especially for people at higher risk.” I believe this positioning is
dangerously complacent and sends the wrong message to those responsible
for guiding us through public health challenges.
"As we approach a new presidential administration and a new Congress,
we cannot regard COVID-19 as one of several respiratory diseases that
can be dealt with through a vaccination program and other
measures. COVID-19 requires special attention from the new
administration, federal health agencies and lawmakers. They need to
remember and treat COVID-19 as having different characteristics compared
to other respiratory diseases and manage it for what it is — a virus
that caused the most extended pandemic in over a century, with a
significant death toll that continues to take lives every day.
"Our knowledge of the disease continues to evolve. We still do not
fully understand it or the best way to treat it. For example, long
COVID, which is estimated to affect 5.3 percent of U.S. adults
in the U.S. (13.5 million people), poses potentially serious and
debilitating long-term health issues such as fatigue, brain fog and
uncontrolled blood pressure.
"We must not abandon the tools, therapies and strategies we’ve
developed to prevent and fight it. That means we must ensure the
availability of at-home tests, educate the public and medical community
on diagnosis and treatment options (both outside and inside the
hospital), be tolerant of people who still seek to protect themselves by
wearing masks, and continue to support and fund research into new
treatments and vaccines.
"We may be tired of COVID-19 but the number of deaths we are seeing
should not be regarded by our leaders in Washington and in the states as
acceptable. COVID-19 requires ongoing vigilance, early diagnosis,
timely treatment through all the stages of disease progression and
continued research.
"Our political and medical leaders must continue to pay attention to
what we learned from the pandemic and must assure that we all are taking
the needed steps, to protect not only ourselves but also future
generations."
The choice for President is clear. Who would you rather vote for, Donald Trump, a man who has served four years as President and has business experience? A man who has done away with stifling regulations? A man who has called for drilling for oil? A man who has kept prices low? A man who has treated Israel with respect and protection? A man who sanctioned Iran? A man who was tough on our enemies? A man who negotiated the "remain in Mexico" policy and started to build a border wall to keep illegal aliens out? A man who was tough on crime?
Or do you want to vote for four more years of higher prices, higher crime, millions of taxpayer-supported illegal aliens at a cost to us of billions of dollars? Do you want to continue with higher gas prices, no drilling, additional regulations that strangle businesses? How about finding retirement unaffordable? Do you want to see Israel further betrayed and attacked by this soft-on-terrorism mentality? Kamala Harris was at Biden's side the last four years and contributed to the absolute mess we're in now. When asked if she, as President, would do anything differently from Biden, she replied, 'There is not a thing that comes to mind,' If you believe that, right before the election, she has suddenly seen the light and will miraculously reverse everything she & Biden have stood for, then I have a bridge I can sell you.
If the Democrat Party's motto and entire platform has devolved into abortion up till birth, transgender surgeries for kids, millions more illegal aliens at taxpayer expense, and "Trump is Hitler", then good luck to America on November 5.
I don't mind getting two COVID shots per year, but wouldn't you think they could develop vaccines that are powerful enough to work with just one shot? And wouldn't it be nice if people who aren't senior citizens would get vaccinated and wear masks, so seniors don't have to get additional shots?
"Seniors
and people who are immunocompromised should get not just one but two
COVID-19 shots this respiratory virus season. That's the new recommendation from the U.S. Centers for Disease Control and Prevention (CDC).
"People
in these groups should get the vaccines six months apart in order to
stay protected against the disease, the agency's vaccine group recently
agreed.
"Here's what to know about the new advice.
Why the need for more than one shot this season?
"The recommendation follows a summer COVID-19 surge
that led to more hospitalizations among the most vulnerable Americans.
While rates are currently low, health experts are concerned they could
spike again during the holiday season, when people travel more and
gather in larger groups. The guidance went a step further for people who
are immunocompromised due to conditions like cancer; they can receive
three or more doses during this respiratory disease season, depending on
how weakened their immune systems are and their potential exposure to
environments where COVID-19 might be circulating.
“What
we have seen over time is that as more and more of the population has
immunity, the most vulnerable individuals are starting to narrow down,”
says Dr. Yvonne Maldonado, professor of global health and infectious
diseases at Stanford University and a member of the committee that
advised the CDC on the decision. “We know at this point that 70% of
hospitalizations now in the U.S. for COVID-19 are among people 65 and
older, and that 50% occur in those 75 and older. So if we address COVID
in those populations, we are looking at potentially reducing 70% of the
risk of hospitalization from the disease in this country right now.”
"Data
also show that immunity generated by the vaccines wanes after four to
six months, so the additional dose should help to keep older people
protected throughout the year—through not just the fall surge, but also
through the additional peaks that have been occurring with COVID-19. “We
are still waiting to learn the pattern of this disease,”
says Maldonado. “COVID-19 seems to have two peaks a year, but they are
not well characterized yet since the virus hasn’t been around very long.
Giving a second dose gives people the opportunity to not spend so much
time worrying about coverage.”
Does the updated shot work?
"The current mRNA vaccines from Moderna and Pfizer-BioNTech
target the KP.2 variant, and the Novavax vaccine targets the JN.1
variant—neither of which are the dominant version causing infections in
the U.S. right now. According to the latest CDC estimates,
the KP.3.1.1 variant is causing nearly 60% of new COVID-19 infections,
and the XEC strain is rapidly becoming more common, responsible for 10%
of new infections. Those variants appear to spread more easily among
people, although there isn't any evidence yet that they could lead to
more serious disease. That's why boosting immunity with another dose for
those most vulnerable to COVID-19 complications could protect them as
their chances of getting infected potentially increase.
"The
KP.2 and JN.1 variants are still related to KP.3.1.1, since all of them
are Omicron subvariants, so the vaccines should still provide
sufficient protection from severe disease, says Dr. Steven Furr, board
chair of the American Academy of Family Physicians. “I tell [my
patients] that the vaccine does decrease hospitalizations and risk of
death,” he says. “They still might get COVID, but they are much less
likely to get it if they are vaccinated—and if they do get it, it’s less
likely to be severe.”
"That’s
especially true for older people and people with weaker immune systems.
“If you are diabetic, or hypertensive and have multiple problems, COVID
could be enough to tip you over to getting pneumonia, getting really
sick and dehydrated," Furr says. "It only takes one illness to tip your
body over to more morbidity and mortality.”
The need for adequate supply
"Vaccination
rates are still relatively low. But seeing friends or family get
infected remains one of the strongest motivators, says Furr—and he
believes the uptick during the summer is encouraging people to ask for
COVID-19 shots when they get their flu shot. For family physicians,
though, getting enough doses to meet that demand has been a struggle.
For his practice in Jackson, Ala., Furr ordered 100 doses weeks ago, and
they've trickled in slowly. “We used up those first 20 doses in two
days,” he says. “We’re told the distributors don’t have them or they are
on backorder. I don’t know if they are prioritizing other groups, but
it’s been a real frustration with the last two iterations of the
COVID-19 vaccine to get enough supply to meet the need.”
"Furr
says it’s important to ensure that family doctors have enough supply.
“People who are on the fence and aren’t begging to get the shot are not
likely to go to the pharmacy,” he says. “They’re going to walk into
their family physician’s office where during a wellness visit or a
diabetic exam they can talk through the vaccine with their doctor.”
"Those
conversations are also critical for helping people understand what the
vaccines can and cannot do. “The point of [vaccination] has never been
to stop all infections,” says Maldonado. “We’ve never had the aim of
stopping transmission and all infections. The idea was to stop
hospitalizations and stop deaths.”
"Allowing
for additional COVID-19 vaccine doses “allows people to make the best
decisions possible to keep themselves and their loved ones safe from
COVID-19,” CDC director Dr. Mandy Cohen said in a statement. “CDC will
continue to educate the public on how and when to get their updated
vaccinations so they can risk less severe illness and do more of what
they love.”
When there are suddenly fewer COVID stories and fewer people masking, I immediately become even more COVID-cautious than usual. And what with the hurricanes and early voting, when large groups of people have gathered at various sites unmasked, I have to wonder what the outcome will be.
by Alix Martichoux at The Hill - 10/27/24 11:31 AM ET
"(NEXSTAR) – October is typically the calm before the
storm when it comes to respiratory viruses. But health experts say it’s
not time to get comfortable. A surge in flu and COVID cases is likely on
the way, but the timing of the winter wave may be different this year.
"The summer of 2024 saw a dramatic increase in COVID-19 cases for a period that stretched well into September.
“Perhaps a silver lining in that cloud is that the large number of
summer cases may mean that our winter wave is going to be a little
smaller because individuals who were infected in the summer should have
immunity that will take them into December and January,” Dr. Andrew
Pekosz, professor at Johns Hopkins Bloomberg School of Public Health,
said in a media briefing this month.
"Because immunity from a prior case tends to last about three months
on average, and so many people were infected in late summer, we may
start to see the next significant uptick in COVID cases in December,
Emily Smith, infectious diseases and epidemiology expert at GW Milken
Institute of Public Health, predicted in an interview with USA Today.
"How big the wave ends up being depends in part on vaccine uptake.
Last year, few people got the updated booster shot. If that’s the case
again this year, we’re more likely to see widespread and serious
consequences, Pekosz said.
"Uptake rates of the flu vaccine are another concern, he said. The
Centers for Disease Control and Prevention recommends vaccinating
against influenza before the end of October so it has time to take
effect before peak flu season.
"Most of the time, flu activity peaks between December and February.
"Adults over 75 and some between ages 60 and 74 can also get vaccinated against RSV, which is respiratory syncytial virus.
"If vaccine uptake for these looks similar to last year, we could be in for a dangerous winter, CDC Director Mandy Cohen said in a briefing at the end of September.
“If last season is any prediction of this season, that means 800,000
hospitalizations of flu, COVID and RSV,” she said. “We know that these
vaccines can cut the risk of hospitalization in half.”
"On
Tuesday, October 22, 2024, Pepperdine University’s Caruso School of Law
awarded 98-year-old Holocaust survivor David Wiener an honorary juris
doctor degree during a ceremony at the Brock House on the Malibu campus.
The event not only recognized Wiener’s remarkable life and resilience
but also celebrated his lifelong dedication to Holocaust education.
"Though he survived the horrors of Auschwitz and several labor camps during World War II, as recounted in his memoir Nothing to Lose But My Life,
Wiener’s parents and all but one of his siblings were killed by the
Nazis. Wiener immigrated to the United States in 1946, where he built a
thriving upholstery business. Alongside his wife, also a Holocaust
survivor, he contributed to various charitable organizations, including
the Boys and Girls Club of Fontana, the US Holocaust Museum, and
Hatzalah Israel. Wiener’s life of philanthropy and dedication to justice
reflects the core values of Pepperdine, and the ceremony underscored
the enduring importance of Holocaust remembrance. ...
“Though
David’s life story is extraordinary, the reason we are awarding him an
honorary law degree today goes beyond mere survival—it’s about what he
did with that life once it had been saved,” shared [Dean Paul] Caron.
"While
David Weiner might not have attended the Caruso School of Law, he
exemplifies the values we seek to instill in our students: wisdom,
creativity, perseverance, selflessness, and an unwavering commitment to
justice for all. If he could overcome the horrors he lived through as a
boy to become the man he became, then each of us should be inspired to
dream a little bigger, to work a little harder, and to be a little more
grateful for the many blessings the Lord bestows upon us each day."
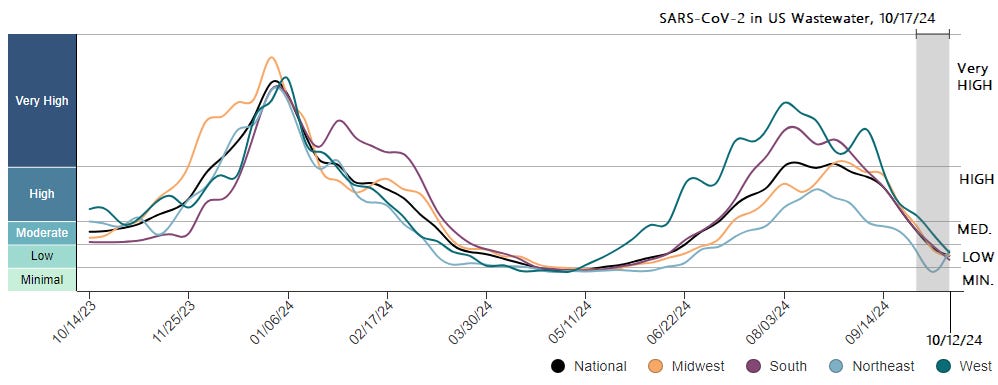
"Wastewater levels of SARS-CoV-2 are LOW
nationally. Last week's uptick in the Northeast has resolved according
to CDC data. According to Sara Anne Willette’s composite wastewater data
from both NWSS & WastewaterSCAN, Montana, Vermont and New Hampshire wastewater COVID levels are HIGH
as of October 22, 2024. Most wastewater locations are only reporting a
few times each week, so it is important to look at the date of the map
in order to know if it is the most recent information. Also, there are a
lot fewer sites reporting wastewater levels of virus now, which makes
it more challenging to get good information. I wrote this post earlier
today on “How to look up SARS-CoV-2 wastewater data in your area” which gives specific SARS-CoV-2 information about U.S. states and about other countries as well.
"Emergency room visits
for COVID in the U.S. have gone down considerably. According to JP
Weiland, we are at a lull for cases, but COVID case numbers are expected
to start to increase in early November. There are approximately 216,000 new COVID infections per day and 1 in every 154 Americans is currently infected. JP Weiland said that he believes that the December 2024 winter wave will be significantly lower than the recent summer wave in the West and in the South. He expects that the Northeast and the Midwest
will have winter COVID waves that will be higher than their 2024 summer
wave, but that their 2024-2025 winter COVID wave will have fewer cases
than last year’s.
"In the United States, the proportion of KP.3.1.1 has remained at 57% of new COVID cases for the last several weeks. Recombinant variant XEC
increased from 2% to 5% to 10% to now 17% of COVID cases over the last 4
weeks. XEC is increasing in many other countries as well and is
expected to become the dominant variant.
"A new article from Yunlong Cao’s lab shows that these variants have special mutations, the S31del mutation of KP.3.1.1 and the T22N mutation of XEC,
that allow them to add glycans to the Spike protein N-terminal domain
(NTD). The additional NTD glycosylation appears to increase the ability
of these variants to evade neutralizing antibodies.
Acute COVID infections, General COVID info
"In a large study of 28,966 immunocompromised adults admitted to the hospital for acute COVID infection between December 2021 and February 2024, iv Remdesivir
significantly decreased mortality in people not on supplemental oxygen
and also in those requiring supplemental oxygen. When stratified by
immunocompromising conditions, "Remdesivir was also associated with
lower mortality in subgroups of patients with cancer, hematological
malignancies (including leukemia, lymphoma, and multiple myeloma), and
solid organ/hematopoietic stem cell transplantation."
"A review of 31 studies looking at COVID transmission on airplane flights
showed that there were sporadic clusters of COVID spread usually to
people seated within 2 seats in any direction of the COVID infected
people. Masking reduced the risk of COVID transmission.
Pregnancy
"A study from Shanxi Province, China found that maternal COVID infection during early pregnancy may increase the risk of congenital heart defects in newborns. In 119 pregnant individuals infected with COVID, 10.1% of their newborns had cardiac abnormalities, compared to 4.1% in the control group. In all but one of the cases, the pregnant person was infected with COVID early, before 8 weeks of pregnancy.
The study also found a significant rise overall in congenital heart
disease during the pandemic, peaking at 5.5% in 2023. "The significant
increase in congenital abnormalities during the COVID-19 pandemic,
particularly the early gestational infections associated with specific
types of cardiac abnormalities, emphasizes the need for ongoing
monitoring and support for children born during the pandemic," the
authors concluded.
"Two
new studies, one from England and one from Kaiser Northern California,
show that babies have a high likelihood to be hospitalized for COVID
infection. The English study analyzed EHR records from 45,000 children
who were admitted to the hospital for COVID infection between July 2020
and August 2023. Babies under age 1 were most likely to be admitted to the hospital for COVID
and represented 43% of all pediatric hospital admissions over the three
year period (July 2020 to August 2023) and 64% of pediatric COVID
hospital admissions between August 2022 to 2023. For older children over
age 1, the severity of hospitalizations, including critical care,
decreased over time, and cases of pediatric inflammatory multisystem
syndrome (PIMS-TS) dropped significantly. Infants under age 1 are the only age group where COVID hospital admissions did not decrease over time.
The findings highlight that infants remain particularly vulnerable to
respiratory illnesses like COVID-19 due to low immunity levels. Infants
are not eligible to be vaccinated, so it is especially important to
vaccinate pregnant individuals against COVID.
Photo: Freepik
"Like
the findings in the English study above, a new study from Kaiser
Permanente Northern California (KPNC) of 1,107,799 children of whom 423
were hospitalized for COVID, found that babies under age 6 months were most likely to be hospitalized for COVID infection.
Pediatric hospitalization rates were found to increase with each new
SARS-CoV-2 variant. In children under 6 months of age, the incidence of
hospitalization per 100,000 person-months increased from 7 during the
pre-Delta period to 22.4 during the Omicron period. Black and Hispanic children, as well as kids with comorbidities, were at a higher risk of hospitalization. Teens
were more likely to be admitted to ICU care. The authors conclude that
"To prevent severe disease in children and adolescents, everyone
eligible should be vaccinated."
Vaccines
"In
America, everyone over age 6 months is eligible for one dose of the
2024-2025 COVID vaccines. The CDC just updated their advice regarding
certain groups. People ages 65 and older should get a second dose of vaccine approximately 6 months after their first. Moderately to severely immunocompromised people
of any age can now get two or more doses of the updated COVID vaccine
per year under shared clinical decision making with their clinician.
“The recommendation acknowledges the increased risk of severe disease
from COVID-19 in older adults and those who are immunocompromised, along
with the currently available data on vaccine effectiveness and year-round circulation of COVID-19.”
Novavax
"The FDA has put the clinical trials of Novavax’s combined COVID-Influenza
and its stand alone Influenza vaccine on hold after a trial participant
reported nerve damage after receiving the combined vaccine.
Vaccines and Mucosal Immunity
"The
entry point of the SARS-CoV-2 virus is often through the nasal mucosa.
This week, there were two new articles in Science magazine about mucosal
immunity in the nose after COVID vaccination. The first article by
Lasrado et al. showed that the XBB.1.5 mRNA intramuscular vaccine from
last winter substantially increased neutralizing antibodies in the
blood, but did not increase mucosal IgA antibody levels in the nose.
"The
second study showed that intramuscular mRNA COVID vaccines can increase
mucosal immunity against SARS-CoV-2, but not in the expected way.
Usually, IgA antibodies are made in nasal mucosal tissues, but in this
case, antibodies found in the mucosa were actually IgG that migrated from the bloodstream into the nose.
Other studies have shown that giving a nasal spray booster vaccine
after mRNA intramuscular vaccination causes an increase of IgA
antibodies against SARS-CoV-2 in the nasal mucosa which can help to
block infection.
"Vaccine expert Dr. Vipin Vashishtha
tweeted, “These differing results by two studies may be due to the
number of SARS-CoV-2 vaccinations or exposures, time since last
exposure, and experimental approaches, but this pair of papers
underscores the need to better understand the mucosal immune response in
humans.”
"To figure out the pathophysiology of SARS-CoV-2 spread in the body, and to understand possible viral persistence
in post-acute COVID, scientists from France used a radiolabeled
antibody to SARS-CoV-2 which they used to follow viral spread over time
using Immuno PET scans
in monkeys. Three months after SARS-CoV-2 infection, the researchers
also found persistent SARS-CoV-2 antigens in the lungs and brain of the
non-human primates on repeat PET scan. Histopathology confirmed these
findings.
"Two patient-researchers with Long COVID, Julia Moore Vogel and Charlie McCone,
wrote a piece in STAT news about the difficulties living with Long
COVID, especially since there are no FDA approved treatments and since
research is moving very slowly. 400 million people worldwide are
suffering immensely from the disease. They recommend that until there
are FDA approved treatments, health care providers should allow patients to try off-label drugs
that have helped other people with Long COVID. They recommend
guidelines and education about Long COVID for doctors regarding which
off label treatments are most helpful for Long COVID symptoms.
"Two groups from the University of California have developed a way to repair genetic mutations before birth to potentially stop neurodevelopmental genetic conditions
like Angelman and Rett syndromes. Using lipid nanoparticles (LNPs), the
researchers were able to deliver Cas9 mRNA to 30% of fetal brain cells
in mice which allowed the disease mutations to be repaired. This
innovative treatment may some day help treat genetic disorders in-utero,
preventing severe disease from developing after birth. “The
implications of this tool for treating neurodevelopmental conditions are
profound. We can potentially correct genetic anomalies at a foundational level during critical periods of brain development,” said the study’s senior author Aijun Wang, a UC Davis professor of surgery and biomedical engineering.
"The FDA recalled 7,107 bottles of Cymbalta (Duloxetine)
made by Towa Pharmaceutical Europe this week as the medication could
cause "temporary or medically reversible adverse health consequences."
Cymbalta (Duloxetine) treats depression, anxiety and chronic nerve pain.
It is important NOT to stop Cymbalta without tapering off of it as that
could cause withdrawal symptoms including severe vomiting.
"Walking pneumonia is a bacterial respiratory infection caused by Mycoplasma pneumoniae. Cases have been increasing since last spring and remain high, especially for young children ages 2-4 years which is unusual.
Forget about the World Series. I was watching a much better match-up last night: Israel vs. Iran! Despite all the continual attacks by Islamic terrorists, surrounded by Arab countries whose goal is the destruction of Israel and all Jews, even though they are outsized 100:1, there was courageous little Israel, retaliating by flying precision bombing missions over Iran, attacking military targets (but unfortunately not the oil refineries). And unlike Hamas, Hezbolleh, Iran, Lebanon, Syria & the rest, Israel doesn't deliberately target civilians.
Biden and Blinken can say "Don't" and call for ceasefires all they want. I think Israel is done listening.
Israel may be tiny, but her courage is huge and her will to survive is stronger than anything these antisemites and murderers can throw at her.
Score: Israel 1. Iran, the Middle East, & the White House 0.
"The eye-watering financial cost of the migrant crisis
hit $150 billion last year and is causing devastating consequences for
residents of hard-hit cities struggling to cope with the influx, The
Post has learned.
"Of that figure, calculated by Washington DC-based non-profit
Federation for American Immigration Reform (FAIR), $67 billion came from
the federal government, but the majority of the burden was shouldered
by states and local governments."
Julia Doubleday, who writes powerful articles about COVID at The Gauntlet, now has a firsthand account of her own struggle with Long COVID. If after reading about her ordeal you still think COVID is "just a cold" and shrug it off, then there's no hope for you.
"A few years ago, I learned that a person who is drowning doesn’t
appear to be drowning. A drowning child generally won’t flail wildly and
scream for help; instead, you’ve got to look for the silent kid. All
the remaining energy of a drowning person is being used to keep
themselves above water, until nothing remains.
"When I’m
having my better days, I’m able to write. Not just here on Substack, but
on twitter, on Instagram, on every fresh newborn Bluesky and ancient
moldering Facebook. Occasionally, reluctantly, I make a TikTok video,
although I dislike being on camera. When I’m working on a reported piece
for The Gauntlet, I’ll have dozens of tabs open-
studies, articles, commentary from researchers, my twitter bookmarks
(chock-full of more studies, articles, commentary from researchers). In
my way, in all the ways I know how, I’m trying to get some help.
"Even on my good days, I’m mostly homebound and rarely out of bed. But
when my symptoms are cooperating, I am at least able to read, write,
watch videos, and share information. I like to think of my mother
telling me, “You might as well do something while you’re doing nothing,”
and I do.
"Although I am sick now, I am still the advocate I was
before I developed Long COVID, before I ever contracted COVID. The
advocate I was because I knew then what I know now: that letting the
virus spread unchecked is unsustainable, based on a poor understanding
of what we know about SARS-COV-2, unjust, and morally wrong.
"But when my symptoms become too severe, one by one, you can watch the lights go out on my accounts. The Gauntlet,
being the place that requires the most work and energy, is the first to
go down. Know that when I can be, I am here. Know that when I stop
screaming for help, I am drowning.
"My most recent
good day was a little over a month ago, on September 20. On that day I
left the house, had a coffee in the park with a friend, and had a conversation with Walker Bragman
on this platform. That Friday capped three weeks of relatively improved
health for me; I was cautiously optimistic. But toward the end of my
90-minute talk with Walker I began to feel tired, distracted, and
headache-y. I lay down, but the next morning I woke up back in a crash.
"For
the next two weeks I continued writing as my symptoms worsened. For me,
Long COVID manifests as a mixture of otherworldly fatigue and endless
headaches. I have the dreaded symptom called “PEM” or post-exertional
malaise, which is characteristic of ME/CFS and afflicts about half of
people with Long COVID. PEM is easy to explain but difficult to
understand and harder to navigate; essentially, any exertion (physical
or mental) leads to a worsening of symptoms, usually 24-48 hours later.
"Finally,
during the week of October 7, I didn’t have a single day with a few
hours’ worth of energy to give to sitting and writing. “I’m no longer
asking,” said my body. Teary, pouty, angry, an absurd, wrathful fetal
position-ball with a bright pink migraine cold-cap on my head, I
admitted defeat and stared at the wall. “You can’t hurry recovery from
PEM,” goes the old saying, “no, you just have to wait.”
"On October
11, I made the mistake of going to a doctor’s appointment while still
in my crash. October 12 and 13 were some of my worst days yet, with
severe migraine that wouldn’t respond to my top-shelf migraine abortive
medication, Ubrelvy, and fatigue that left me fully bedbound. Last week a
friend did my laundry for the first time, then my dishes, and took out
my trash. While she cleaned around me, I lay in my bed, in my strange
mix of feelings: gratitude and love for my friend, fear for my future,
defeat for my present, plus a weird swirl of humiliation that is, I
suppose, internalized ableism.
"Long COVID crashes turn me into a
detective, a researcher, an archivist. I remember the days I did and
didn’t get out of bed, the days I did and didn’t have a migraine. I
develop theories and debunk them, read the studies coming out and try to
understand them. I update my friends about my condition in minute
detail, the way people talk about their new baby or their dog (if
they’re a little too into their dog). I know I’m probably boring them. I
think they miss the me I was before, and I miss her too. I miss being
able to dress up. I miss being able to have a cocktail. In my crash, I
can’t even have caffeine, and I long for the simple comfort of a hot cup
of coffee in the morning.
"It’s important, they say, to relax
when you’re crashing; I worried about everything. If you engage with
Long COVID spaces at all, you’ll know there is always a contingent of
patients scolding people for “negative thoughts”, and I had negative
thoughts about those people. On top of my worrying, I worried about my
worrying; what if it really is making me worse? Should I really be on a
no-carb diet? (Way too hard, I decided; half my calories are coming from
energy bars). I worried about how sick I am, I worried about how long
it would be until I could leave my home again (I still haven’t). I
worried about my finances. And relatedly, I worried about when I’d be
able to write again. I’m not well enough to have another job nowadays.
"At
one point I turned to twitter, migraine and all, to beg for advice: I
asked whether anyone with PEM had improved on any medication, and if so,
what med? I also asked if anyone knew of Long COVID competent doctors
in DC who accept insurance. Most of the responses were kind, but of
course, there’s no magical cure for PEM, only people who seem to have improved somewhat on medications that may or may not
work for others. One person tells me to pace, and I explode in
frustration. “All I do is lie in bed all day! I can’t pace more than I’m
pacing!” He then recommends thinking good thoughts, and reader, my
thoughts are not good. Desperation pushes me once again to buy
supplements that, I’m reasonably sure now, are doing nothing. I’m still
waiting to see specialists, who are booked out for months. My PCP is
caring, and listens to me, which is a best-case scenario for Long COVID.
She orders tests and follows up on them. I don’t get any better.
"This
week, for some reason, I’ve slightly improved. Rather than attributing
it to any foods I ate, thoughts I thought, or expensive supplements I’ve
added to my 15-supplement regimen, I know now to blame it on nothing
more than chance, and likely rest. I have rested, but I don’t feel rested;
more like I’ve been struggling on the open ocean when suddenly,
miraculously, and utterly randomly, I find myself washed up on the shore
of some desert island. Beaten up, bedraggled, bedridden still, but
suddenly breathing.
"I am not well enough to walk and get a
coffee, or do my laundry, or leave my apartment. But I’m well enough to
shout for help, so I’m here. Thank you for being here too."
"The Centers for Disease Control and Prevention (CDC) vaccine advisory
group today recommended a second 2024-25 COVID-19 vaccine dose, spaced 6
months apart, for people ages 65 and older and for people in younger
age-groups who have moderate or severe immunocompromising conditions.
"The
group also recommended an extra dose, three or more, in people with
immunocompromising conditions, based on shared decision-making between
patient and doctor.
"The recommendation replaces a vaguer
"additional doses" wording that the Advisory Committee for Immunization
Practices (ACIP) used in its advice over the summer for at-risk groups
for the 2024-25 vaccines. The group made the change to simplify and
standardize language used for its routine immunization schedules.
"The three-part vote passed unanimously.
Challenges in maintaining protection
"The ACIP work group that
proposed the recommendation grappled with several factors, including a
lack of seasonality of SARS-CoV-2 circulation, the epidemiology of the
disease, waning vaccine effectiveness, and variant changes.
"Vaccine
timing has become complex, especially given tough-to-predict waves
involving new COVID variants that sometimes spike in warm-weather
months, after protection from vaccination in the fall months has waned,
but before updated vaccines arrive on the market. For example, over the
past spring and summer, COVID activity circulated at a high level over
many months.
"Hospitalization rates from COVID remain higher in seniors, especially those ages 75 and older.
"According
to the CDC's latest data for the last respiratory disease season, 40%
of adults ages 65 and older received one dose of the vaccine and 8.9%
received a second dose, with second-dose levels higher in people in
urban areas and in certain geographic regions. CDC experts told the
group that a healthcare provider recommendation helped sway patients to
receive a second dose.
"Meanwhile, second-dose coverage in immunocompromised people ages 18 and older was lower, at 5.4%.
Extra flexibility for immunocompromised groups
"Also,
along with the general two-dose recommendation for immunocompromised
people ages 6 months to 64 years, in a move to create more flexibility
with COVID vaccination, ACIP recommended additional doses—three or
more—of the 2024-25 vaccine in people ages 6 months and older who are
moderately to severely immunocompromised with shared clinical
decision-making.
"CDC experts recommended a minimal 2-month
vaccination interval to allow for flexibility based on the patient's
risks and circumstances.
"The CDC director considers ACIP recommendations before making a formal recommendation."
I'm glad to see these guidelines repeated for people who ignore them, but unless I'm missing something from past years, just what has been updated? It's unfortunate, but these "guidelines" just look like suggestions that most people won't even follow anyway.
"CINCINNATI (WKRC) — As winter approaches, the Centers for Disease
Control and Prevention (CDC) has updated its guidelines to help reduce
the spread of COVID-19 and other respiratory viruses, such as the flu.
The CDC now suggests getting an updated flu and COVID-19 vaccine each
year.
"Jennifer Wick, director of ambulatory pharmacy at Christ Hospital,
said, "While the flu shot may not 100 percent prevent you from getting
the flu, it will prevent you from getting the more serious
complications."
"If you do get sick, the CDC advises that
regardless of which illness you test positive for, if you have a fever,
you should stay home until it has been gone for at least 24 hours and
your symptoms are improving. Afterward, wearing a mask is suggested for
the next five days. During this period, it is also recommended to test
to ensure your illness is gone, stay away from people most at risk for
illness, maintain good ventilation, and wash your hands frequently. This
is because you can still spread a respiratory illness even when you are
feeling better.
"The CDC also notes that vaccinated individuals are less likely to
transmit a virus compared to those who are not. Wick mentioned that many
patients aim to get vaccinated around October, as virus season runs
from now to March.
"The CDC emphasizes that these recommendations are most critical for
those at high risk for severe illness, such as individuals 65 and older
and those with weakened immune systems. "
At the height of World War II, Anne Frank
spent more than two years cooped up with her family in a secret annex
in Amsterdam. While hiding from the Nazis, the young girl filled the
pages of her now-iconic diary.
For decades, travelers have been able to see the Frank family’s hideout by visiting the Anne Frank House,
a biographical museum created in the 1950s in collaboration with her
father, Otto Frank. The Amsterdam museum is one of the most famous
historical sites in the Netherlands, welcoming more than 1.2 million visitors each year.
Now, for the first time ever, a full-scale replica of the secret annex will open on foreign soil. “Anne Frank the Exhibition”
will debut at the Center for Jewish History in New York City on January
27, 2025—which is also International Holocaust Remembrance Day. The
show will mark the 80th anniversary of the liberation of Auschwitz.
The 7,500-square-foot, one-story exhibition will take visitors on a
journey through time, starting with Frank’s childhood in Frankfurt.
Using more than 100 original artifacts and multimedia elements, it will
also explore the Nazis’ rise to power and Otto Frank’s experiences
during the postwar years.
The real secret annex in Amsterdam is empty, per Otto Frank’s
request. But the New York replica will be outfitted with some of the
Franks’ furnishings.
“We feel that this will bring audiences who are not necessarily
familiar with the story closer to that history and closer to Anne
Frank,” Ronald Leopold, the Anne Frank House’s executive director, tells
the New York Times’ Laurel Graeber.
After the replica annex is constructed in the Netherlands, it will be
shipped across the Atlantic to New York. Frank’s famous diary will not
be making the journey.
“We unfortunately will not be able to travel with the diary,
writings, the notebooks and the loose sheets that Anne wrote,” Leopold
tells the Associated Press’ Mike Corder. “They are too fragile, too vulnerable to travel.”
Frank was born in 1929 in Frankfurt, Germany, to parents Otto and Edith Frank. Less than four years later, Adolf Hitler became Germany’s chancellor and began orchestrating what became known as the Holocaust.
The Frank family moved to the Netherlands to escape persecution in
the mid-1930s. In July 1942, the Nazis ordered Anne’s older sister, Margot, to return to Germany and report to a labor camp. Instead, the family went into hiding.
Their hiding spot was the secret annex at Prinsengracht 263, where Otto Frank ran his pectin-trading business. Soon, they were joined by the van Pels family and dentist Fritz Pfeffer,
which brought the total number of people in the cramped space to eight.
The group remained there for more than two years, with colleagues and
friends supplying food, clothing and reading materials.
On August 4, 1944, police raided the annex and arrested all of its
occupants. Anne and Margot Frank were sent to the Bergen-Belsen
concentration camp, where they died around March 1945. Edith Frank died at the Auschwitz-Birkenau concentration camp in January 1945.
Otto Frank was the only member of the family to survive. After the
war, Miep Gies, one of the helpers who had hidden the family, gave him
Anne’s diary and writings.
“At first, he could not summon the courage to read them, but once he started, he was gripped by her writing,” according to the Anne Frank House.
He began sharing passages with family and friends. Two years after
the war ended, her diary was published in Dutch and eventually
translated into many other languages.
The exhibition will explore Anne Frank’s lasting legacy “not just as a
victim, but through the multifaceted lens of a life, as a teenage girl,
as a writer, as a symbol of resilience and of strength,” Leopold tells
the AP.
“We hope that [visitors] will contemplate the context that shaped her life,” he adds.
“Anne Frank the Exhibition” will be on view at the Center for Jewish History in Manhattan, New York, from January 27, 2025, to April 30, 2025.
Here's a familiar headline that shows the Biden Administration's desperation to get a ceasefire to help Kamala Harris in time for the election. Sorry, this shameless 11th attempt won't work either!
Why would Israel trust him, especially after the leak of Israel's plans against Iran? I would tell Blinken to turn around and go back to Washington, or else refuse to meet with him in person.
“In all likelihood, the Biden-Harris administration has prolonged the
Gaza war, allowed aid to flow to Israel’s enemies, and misused taxpayer
funds,” Senator Tom Cotton recently warned USAID
Administrator Samantha Power. “You should immediately suspend all aid
until taking credible and serious steps to stop Americans’ tax dollars
from funding terrorists.”
That will never happen as long as they need Israel to be the villain and the "Palestinians" to be the victims.
COVID news & more, 10/19/24, byRuth Ann Crystal MD, Oct 19, 2024
Wastewater SARS-CoV-2 levels nationally are LOW
and are continuing to descend in all regions except for in the
Northeast where there has been an uptick. No states are in the VERY HIGH
level of wastewater virus at this time. According to the CDC, Minnesota, Missouri, New Hampshire, Vermont and Wyoming have the highest
levels of wastewater SARS-CoV-2 virus, followed by high levels in
Arizona, Maine, and Oregon. Here in California, wastewater COVID levels
are low across the state.
Pseudovirus testing from Kei Sato’s lab shows that the XEC
variant is somewhat more immune evasive and infectious and therefore it
is expected to be the next dominant SARS-CoV-2 variant globally. XEC
has modest growth now, but it is not expected to cause as big of a wave
as recent variants did. The new COVID vaccines are available and they
should protect against XEC and KP.3.1.1. If you have not received your
fall vaccine yet, you may want to consider waiting until mid-November so
as to boost immunity right before Thanksgiving and Christmas. Remember,
it takes at least two weeks after vaccination to make enough antibodies
for good protection.
Emergency department
visits for COVID have significantly decreased compared to a few months
ago, but are not yet as low as levels seen in April this year.
Fortunately, emergency department visits for COVID are less than half of what were seen in the fall season in 2022 and 2023.
UK
“Covid infection levels in England have risen by 17%
last week, with around 1 in 91 people in England now infected with
COVID as of 13 October… COVID infection levels in England have increased
steadily since the middle of August and are now just below the levels
seen in the July peak.”
France
France
had their highest summer COVID wave ever this year. Within the last
month, there has been a steep increase in COVID infections among people
over the age of 65 in France.
A
new study from the University of Kentucky studied 120 patients
hospitalized with critical COVID of which 98 patients (82%) required
mechanical ventilation for a median duration of 14 days. Ninety-three
percent of these patients had generalized fatigue and exercise
difficulties in the short term. Eleven of these patients agreed to be
followed long-term and underwent a muscle biopsy 267 ± 98 days after discharge. Skeletal muscle tissue from critical COVID recovered patients showed increased M2-like macrophages and satellite cells and lower mitochondrial complex II and complex IV activity compared with controls.
From March 2020 to May 2023 during the pandemic, excess deaths
were highest for American Indian/Alaska Native, Pacific Islander, and
Hispanic populations. Surprisingly, the largest relative increase in
mortality was in a younger than expected population- adults aged 25 to
64 years. Among people ages 25 and under, 51% of the excess deaths
occurred in the Black population.
Pregnancy
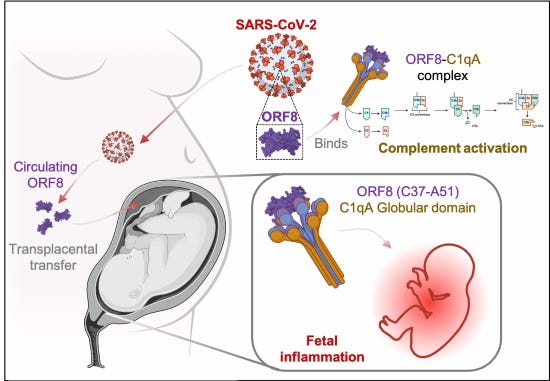
Prenatal
SARS-CoV-2 infection is linked to higher pregnancy and birth
complications, with strong inflammatory responses found in both mothers
and their babies. Researchers from Cleveland Clinic found the SARS-CoV-2 viral protein ORF8
in 60% of fetal tissues (placenta, amniotic fluid, umbilical cord
sample), even though only 26% tested positive for the virus' RNA. The
viral ORF8 protein in the fetal tissues led to inflammation and
activation of the complement system, suggesting that this protein contributes to fetal inflammation during COVID-19 pregnancies, even without direct viral infection.
Adults
have been found to have an increased risk of Type 2 diabetes after
COVID infection. In a new retrospective study of 613,602 pediatric
patients aged 10 to 19 years, there was an increased risk of Type 2 diabetes after COVID infection that was not seen in kids with other respiratory infections (ORI).
Teens and kids who had a COVID infection had a 48-58% increased risk of
Type 2 diabetes. Those who had obesity or were overweight had double
the risk of Type 2 diabetes as compared to kids with ORI. Teens and
children who were hospitalized with COVID had a 2.6 to 3.1-fold risk of
getting Type 2 diabetes after their COVID infection.
COVID is not benign for children. A new piece in Scientific American shows that 10-20% of children infected will get Long COVID,
often with symptoms such as cognitive difficulties, memory issues,
pain, and fatigue. On last estimate, 5.8 million American children have
Long COVID, which can impact nearly every organ system and contribute to
both learning and behavioral challenges. Repeat infections have been
found to increase the risk of Long COVID in adults and probably does in
children as well. It is important to protect kids with vaccination,
improved air quality in schools, and better health policies such as
staying home when sick.
Masking and COVID precautions such as social distancing earlier in the pandemic appear to have made a type of flu, Influenza B/Yamagata, to become extinct.
The CDC still recommends a flu shot for everyone over 6 months of age.
The latest flu vaccine will be trivalent instead of quadrivalent, and
will protect against Influenza B/Victoria and two influenza A lineages
that are circulating.
China's
strict "zero-COVID" policy involving prolonged lockdowns for much of
the population was abruptly lifted in December 2022. Ninety percent of
Chinese people were vaccinated with inactivated virus vaccines like
Sinovac prior to reopening. The rapid reopening led to a massive surge
in infections, with 80% of the Chinese population contracting the
Omicron variant of COVID shortly thereafter.
Risk
factors for Long COVID were found to include female sex, Northern China
location, chronic health conditions, smoking and alcohol consumption.
Vaccination, especially with booster doses, significantly reduced Long
COVID risk. Of note, people who had a COVID infection reported increased
bacterial, influenza and mycoplasma infections as well. Approximately 9% of people reported new onset chronic diseases after a COVID infection.
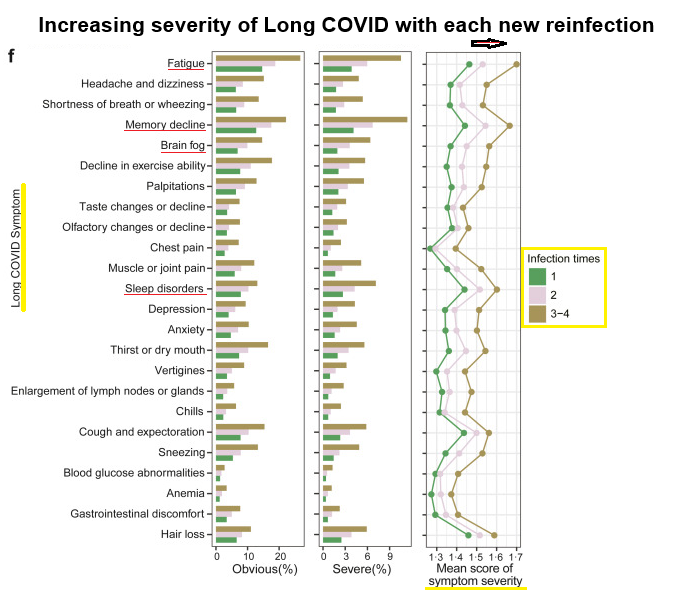
Dr.
Ziyad Al-Aly wrote a commentary on the new Long COVID study from China
noting “despite having milder acute symptoms during reinfection,
participants who experienced multiple infections were more likely to
experience various Long Covid symptoms with greater severity. The
authors show that having two infections is a risk factor for many
long-term Covid symptoms, and the risk increased exponentially when the number of infections exceeded two. These new data on Long Covid risk after reinfection are remarkably consistent with prior studies.”
A
group from Sweden looked at new-onset autoantibodies in 478 healthcare
workers (HCW) with mild to moderate COVID infections and 48 hospitalized
COVID-19 patients at five time points over a 16-month period in 2020
and 2021 using proteome-wide and targeted protein and peptide arrays.
They found a wide array of new autoantibodies
of which 60% remained elevated for at least 12 months after infection.
People with more severe COVID infections were found to have more
autoantibodies. In people with neurological symptoms after COVID, autoantibodies to CALU, MYO16, and SNURF
were noted. CALU is found mostly in the heart and skeletal muscle,
MYO16 is found in the brain, and SNURF is expressed in brain, muscle
tissues and heart muscle cells. The group initially reported their
findings in February 2024 as a preprint in MedRxiV.
Looking
at a different cohort of patients, the same group found autoantibodies
to TRIM63 especially in hospitalized patients and anti-CCDC63 IgG in
people with muscle and joint pain.
"Our results show that prevalent new-onset autoantibodies against a
wide range of antigens emerged following SARS-CoV-2 infection in
relation to pre-infectious baseline samples and remained elevated for at
least 12 months."
A group from Spain evaluated
microvascular damage after COVID infection in people with Long COVID
(aka post-COVID-19 condition (PCC)) by looking at their retinas.
"Retinal microvascular alterations, characterized by reduced retinal
vascular density (VD) and perfusion density (PD) in the superficial
capillary plexus (SVP) and larger foveal avascular zones (FAZ) areas,
were associated with cognitive impairments in post-COVID-19 condition
(PCC or Long COVID) individuals. These findings suggest that severe COVID-19 leads to long-lasting microvascular damage, impacting retinal and cognitive health."
A new study from Stanford of 526 adults with Long COVID shows that 71.9% had persistent moderate to severe autonomic dysfunction at a median of 3 years
post acute infection. 37.5% of these Long COVID patients could no
longer work or had to drop out of school due to their Long COVID illness
and 40.5% were newly diagnosed with postural orthostatic tachycardia
syndrome (POTS). Autonomic dysfunction is highly prevalent in people
with Long COVID.
The Cohen Center for Recovery from Complex Chronic Illnesses (CoRE) at Mount Sinai
just opened as a clinic and research center for people with Long COVID,
as well as ME/CFS, and chronic Lyme's disease. It includes specialized
testing such as tilt table tests, cognitive testing, Metamax and
EndoPAT. In addition, CoRE features an upgraded air filtration system
and far-UVC lighting, and staff wear N95 masks during visits to help
prevent COVID and other infections. The center is run by David Putrino
of Mount Sinai's and by Dr Amy Proal of PolyBio. "Putrino was not an
expert in complex chronic diseases when the pandemic started. His
expertise and position at Mount Sinai focuses on rapid innovation:
speeding up the decade-plus that it typically takes for research to go
from a lab bench to a patient’s bedside."
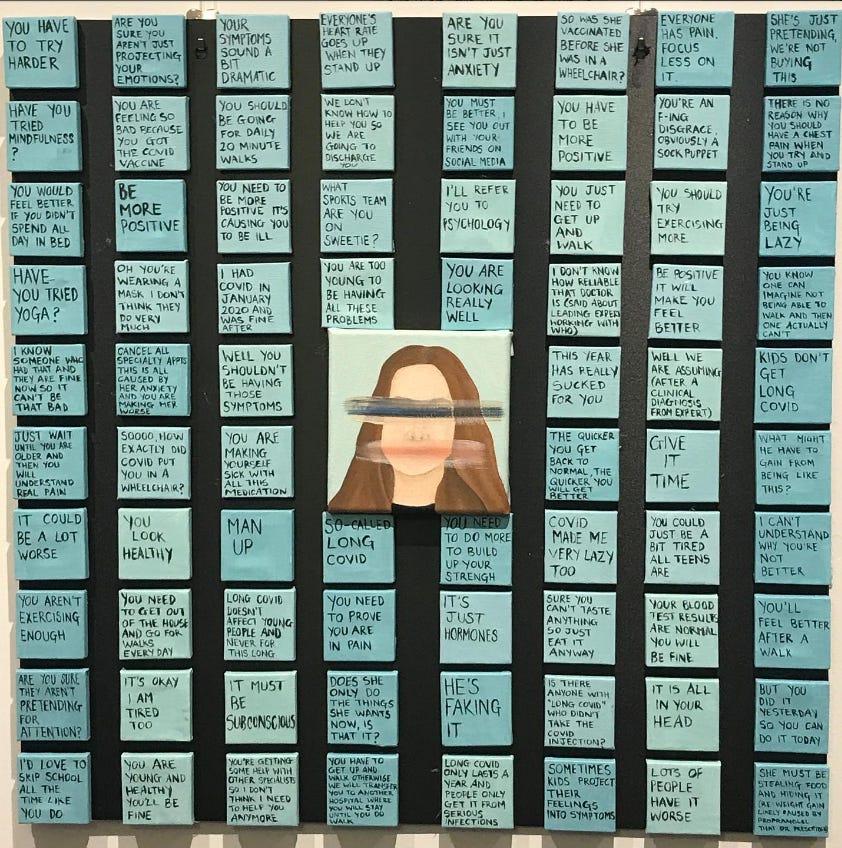
Grant Wakefield made a new 16 minute documentary “about the true nature of SARS-CoV-2 and the impact of Long COVID on one family.”
The film focuses on 17 year old Rosie who has had Long COVID for 3
years. Her art is powerful- expressing the limitations and frustrations
that living with Long COVID causes for both children and adults. The art
piece below is from Rosie
who writes, “It represents how young people with Long Covid lose their
identity and their voice… The words around the edge are all things that
children and young people have been told by their doctors, their
friends, their families and their classmates.”
From: @rosiepidgeonart on Instagram
H5N1
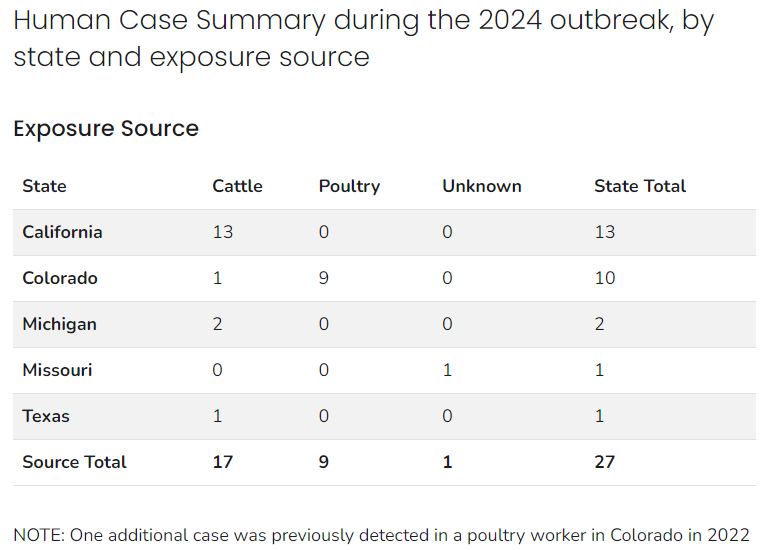
As of yesterday, the California Department of Public Health (CDPH) reported “a total of 13 human bird flu cases have been confirmed in California.
All 13 cases are Central Valley individuals who had direct contact with
infected dairy cattle and were confirmed after additional testing by
the Centers for Disease Control and Prevention (CDC).” If you test for
it, you will find it.
Patients with GIP and GLP-1 RA
medication prescriptions like Mounjaro and Ozempic, which are typically
used for weight loss and diabetes glucose control, were found to have
40% lower rates of opioid overdose and 50% less alcohol intoxication in a
new study.
Good news- the Marburg virus outbreak in Rwanda is
under control. There have been no new cases (total of 62 cases), no new
deaths (total of 15 deaths), only 3 people still receiving treatment
and 59 people have recovered. Over 1,000 vaccine doses have been given
to people in the area.























.jpg)