-----------------
The summer wave of COVID infections has started. As of June 25, 2024, the CDC estimates that COVID-19 infections are growing or likely growing in 44 states, declining or likely declining in 1 state (Hawaii), and are stable or uncertain in 5 states and territories.
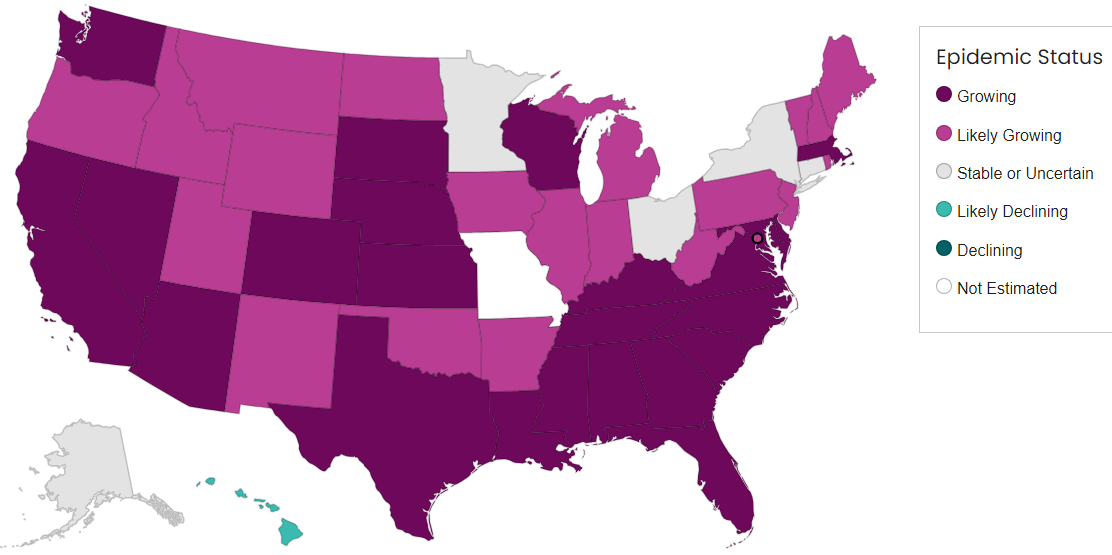
From https://www.cdc.gov/forecast-outbreak-analytics/about/rt-estimates.html
According to Michael Hoerger, Americans will get 500,000 to 600,000 COVID infections each day which means that 187,000 new people will end up getting Long COVID each week over the summer. COVID transmission in late June 2024 is 2x higher than in June 2023, 3x higher than in June 2020 and 5 to 6x higher than in June 2021. In June 2022, the BA.2 Omicron surge surpassed all prior summers.
Nationally, SARS-CoV-2 test positivity is up to 8.6%, emergency department visits for COVID and COVID deaths are increasing. Hospitalizations are no longer reported for most places in the US, but those that are reporting show an increase in hospitalizations for COVID. Tests done at Walgreens pharmacies show a total COVID test positivity of 34.1% for the people that choose to be tested.
Regarding wastewater monitoring of SARS-CoV-2, the CDC still reports the national level to be “LOW”, although we see on the chart below that the west coast virus levels are climbing, followed by increases in southern states. As the weather gets hotter, more people will need to go indoors into the air conditioning. Also, many people are traveling. JP Weiland reports that as of June 28, every 1 in 43 people in the West is currently infected and that in the South, every 1 in 76 people has COVID now. In the Midwest, 1 in 136 people are presently infected with COVID and in the Northeast it is 1 in every 189 people.
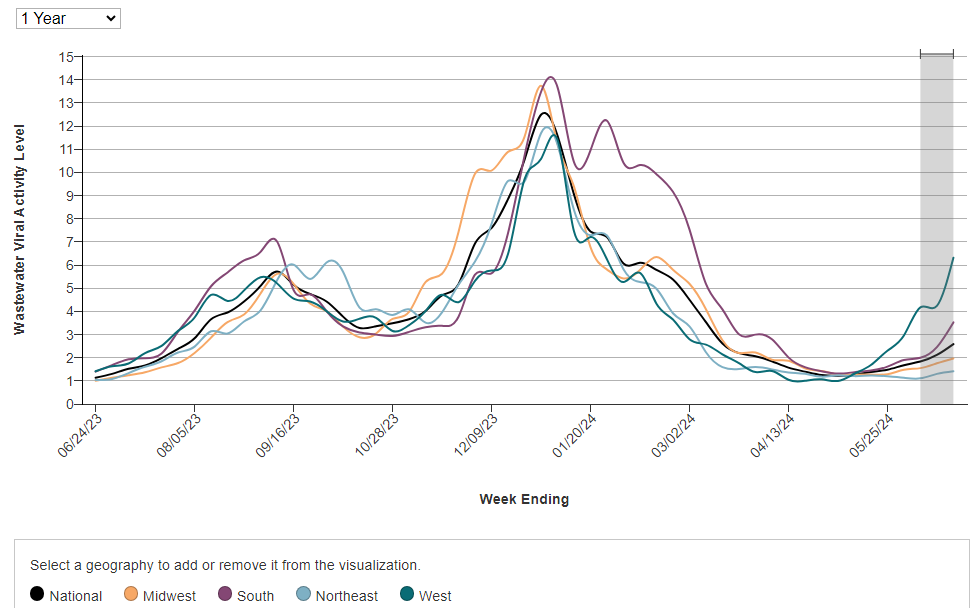
From: https://www.cdc.gov/nwss/rv/COVID19-nationaltrend.html
Regarding wastewater levels of COVID, as of 6/27/24, the CDC reports:
“VERY HIGH” wastewater levels of SARS-CoV-2 are seen in Hawaii, Nevada and Utah, followed closely by Florida and New Mexico.
“HIGH” levels are seen in Missouri, Kansas, Washington state and Maryland, followed by California, Texas, Massachusetts, Louisiana, and Wyoming.
In California, Oceanside San Francisco (1277PMMoV) and Southeast San Francisco (1140 PMMoV) are at the highest SARS-2 wastewater levels, closely followed by Windsor (999). Three of the sewersheds in Santa Clara County are “HIGH” including San Jose which is at 650 PMMoV. Marin county is “MEDIUM”, but with an upwards trend. In Alameda County, Union City was very high at 1096 PMMoV but has now decreased to 428. Oakland is only at 210 PMMoV. In Los Angeles County, SARS-CoV-2 wastewater levels are fairly low still, but are starting to creep up. L.A.’s wastewater is between 81 and 129 PMMoV.
According to Raj Rajnarayanan, the top circulating lineages in California are KP.2.3, KP.2, KP.3.1, KP.3.3. In New York State, often considered the bellwether state, LB.1.7 and KP.2.3 are the top circulating SARS-CoV-2 lineages. COVID hospitalizations are "clearly trending up" in New York. Nationally, COVID variants are only being updated every 2 weeks by the CDC which were noted as KP.3, KP.2 and LB.1 last week.
In her June 25 “State of Affairs” newsletter, Katelyn Jetelina summarized what illnesses to watch out for this summer. She discusses the summer COVID wave, norovirus (stomach flu), whooping cough (pertussis) outbreaks in Delaware and Kentucky and the UK, heat related illness, tick-borne illnesses, and recent mpox infections seen in DR Congo.
Acute COVID infections
This week, Dr. Akiko Iwasaki tweeted about an article by Lindeboom et al. on immune signatures seen in those people who get COVID infections and those who do not. The Lindeboom group infected 16 unvaccinated volunteers who did not have prior COVID infection with a low dose of SARS-CoV-2. While this is ethically problematic given that any infection can cause Long COVID, it does allow us to understand the human immune response to the SARS-CoV-2 virus. Fortunately, none of the participants got Long COVID per Dr. Iwasaki.
Of the 16 unvaccinated people who were infected with SARS-CoV-2, “6 had sustained infection, 3 had transient, and 7 had abortive infection at this dose.” People with a sustained infection had a delay in local IFN I release and cellular immune responses. Volunteers who only had transient infections had rapid IFN-I and cellular recruitment into the nose and throat on day 1. Those who did not get COVID infection (had abortive infection) had higher baseline expression of HLA-QA2 mRNA.
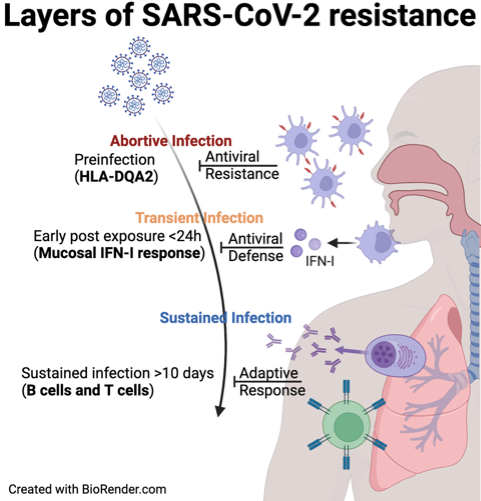
From https://x.com/VirusesImmunity/status/1803466022218854467
An article this week describes a breath test for COVID that is very accurate. However, it is not a point of care test. During the Alpha and Delta COVID waves, exhaled breath samples were collected in 1L Tedlar bags and were then brought to a lab where they were analyzed using a novel silicon microreactor and ultra high-performance liquid chromatography-mass spectrometry (UHPLC-MS). Carbonyl compounds including 34 ketones and aldehydes were evaluated in breath samples. “The model still achieved 90.1% sensitivity, 98.3% specificity and 94.7% accuracy.”
A new cross-study comparison of two large, open-label studies reports that in 2020, giving Remdesivir for patients hospitalized for COVID infection and low oxygen was associated with a 54% lower mortality than the standard of care.
Pediatric Long COVID
In a retrospective cohort study using EHR data from the RECOVER program, 1,864,637 children and adolescents under age 21 were studied from March 2020 and May 2023. Compared to a non-infected control group, kids and teens with COVID infection had a higher risk of adverse kidney outcomes after COVID infection. Children with kidney disease prior to their COVID infection all had worsening of their kidney disease as well.
Using levels of salivary biomarkers TOS, ADA2, total proteins, and AOPP in children, a group from Spain made a model that could predict which children had Long COVID and which were healthy controls. The addition of total proteins and ADA1 levels to the four salivary biomarkers above allowed the group to distinguish which kids had mild and which had severe Long COVID.
Vaccines
The CDC has recommended that all Americans aged 6 months and older receive one of the new fall Covid-19 vaccines. This recommendation comes in response to a summer wave of Covid-19, with infections rising in at least 44 states. The upcoming fall mRNA vaccines will be against KP.2 and the Novavax vaccine will be against older variant JN.1.
Children, especially those under 5, are particularly vulnerable to COVID infections. However, only about 14% of children were immunized against Covid-19 last fall. Many people mistakenly believe the virus is harmless to children. Children are also more likely to bring the virus home to their parents and grandparents. "By immunizing all groups, you're more likely to prevent the spread," Dr. Matthew Daley said.
The fall COVID vaccines will be especially important for pregnant individuals, not only to protect themselves, but also to safeguard their babies until they are old enough to be vaccinated at 6 months of age.
A new “megastudy” in Nature magazine shows that COVID vaccination reminders increase the uptake of COVID vaccines by 21%, with an added benefit of increasing flu vaccination by 8%. The study found that offering free-rides to pharmacies did not increase vaccination more than the behaviorally informed text message reminders.
In 2023 to early 2024, the XBB.1.5 mRNA vaccine was 62% effective against COVID-19 hospitalization and 58% effective against emergency department or urgent care visits. Older versions of COVID vaccines did not reduce the risk of COVID hospitalization, regardless of the number of prior doses received. Therefore, it is important to get updated COVID vaccines to continue to be protected. “The combination of waning vaccine-induced immunity and continuous SARS-CoV-2 strain evolution eventually renders prior versions of vaccines ineffective."
Using single-cell analysis of spike protein (S)–specific memory CD4 T cells after SARS-CoV-2 infection or vaccination, the authors found that the inflammation from COVID infection durably imprinted memory CD4 T cells to be inflammatory. COVID infection primed the T cells to have epigenetic signatures of inflammation, but COVID vaccine primed T cells did not.
Rituxan (Rituximab) is a medication that depletes B cells that make antibodies. Vaccinating people with autoimmune rheumatic diseases before treating them with Rituximab allows them to have a good antibody response to COVID vaccination. If the person already had Rituximab, they will get the best antibody response to COVID vaccination if they wait at least 9 months after their last Rituximab dose to vaccinate.
Mask Bans
North Carolina passed a mask ban, and although it has an exemption for people who need to mask for health issues, anyone can ask the person to remove their mask at any time for “identification”. Now, several other places are considering mask bans. New York Democrats have created a bill that would ban wearing masks for all “assemblies” greater than 5 people. See my notes below for phone numbers to call to request that they stop this bill.
Los Angeles Mayor Karen Bass announced on June 25 that she planned to ban masks at protests. In a twist of irony, Mayor Bass had to move her June 28 meetings to online because she became infected with COVID.
Long COVID
Science magazine reviewed the two recent articles from the Iwasaki group and from the den Dunnen group showing that giving IgG from people with Long COVID to mice caused the mice to get the same Long COVID symptoms. Drs Avindra Nath and Petter Brodin discussed that unlike most autoimmune diseases, there is not one particular autoantibody with the same target in all Long COVID patients. Recent trials show that medications efgartigimod and rituximab that work by decreasing autoantibodies did not improve Long COVID. Dr. Nath is currently studying IVIG for Long COVID.
Long COVID can be very heterogeneous with different phenotypes. Dr den Dunnen proposes using the same mouse study as a biomarker for Long COVID autoimmunity. If you inject a Long COVID patient’s IgG into a mouse and the mouse gets the same symptoms, then that person has the autoantibody-type Long COVID and could be offered a particular clinical trial.
Dr. Iwasaki believes that Long COVID patients with small fiber neuropathy (SFN) pain may be the ones who most commonly will be found to have autoantibodies leading to their pain. She bases this on a recent study by McAlpine et al. That retrospective case series studied 16 patients with new onset SFN after COVID infection. Ninety-two percent of these patients had post-exertional malaise characteristic of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Nine patients had been tested for autoantibodies and six of them were positive for either trisulfated heparin disaccharide (TS-HDS) or fibroblast growth factor receptor 3 (FGFR3) autoantibodies. Eight post-COVID SFN patients were treated with IVIG and had significant clinical improvement in their neuropathic pain symptoms. This study offered preliminary evidence that post-COVID SFN is responsive to treatment with IVIG and linked with neurovascular dysregulation and dysautonomia.
A group from Stanford looked at differences between males and females and at the “immune correlates of Long COVID development, persistence, and resolution”. During the initial COVID infection, females who would later develop Long COVID showed higher levels of XIST, an RNA gene linked to autoimmune diseases. In contrast, males who would develop Long COVID three months later had significant increases in TGF-β signaling in proliferating NK cells during their acute infection. One year after the initial infection, females displayed higher IL1 signaling in their monocytes.
Both males and females with Long COVID had reduced signaling from monocytes and increased activity of NF-κB transcription factors. In both sexes, those with ongoing Long COVID showed higher levels of LAG3, a marker of exhausted T cells, lower ETS1 transcription factor expression across various lymphocyte types, and increased IL-4 levels within T cell subsets. These findings suggest that changes in ETS1 might lead to an abnormally high Th2-like response in Long COVID patients.
A huge study of 10 million people in South Korea and 12 million people in Japan shows a significant increase of neuropsychiatric issues in Long COVID including Guillain-Barré syndrome, cognitive deficit, insomnia, anxiety disorder, encephalitis, ischemic stroke and mood disorders. COVID vaccination protected against these long term symptoms.
A study of 1,988 U.S. Military Health System beneficiaries with Long COVID symptoms identified three Long COVID phenotypes that could be identified by risk factors and early post-infection biomarkers. The sensory cluster (loss of smell and/or taste) had all been outpatients with their initial COVID infection and had elevated ICAM-1 concentrations early after their acute COVID infection. People in the fatigue/difficulty thinking cluster had elevated D-dimer and IL-1RA early after their infections, while patients in the difficulty breathing cluster were more likely to have obesity and have been hospitalized with acute COVID infection.
At Yale, Dr. Harlan Krumholz is working with Dr. Akiko Iwasaki to create a decentralized, national clinical trial that is brought directly to the homes of people with Long COVID. Many people with Long COVID are disabled and would have difficulty traveling to Long COVID clinics. The Yale Long COVID (PAX LC) Trial sends the drug or placebo to the patients' homes. The Long COVID patients can fill out an electronic diary that is uploaded to Yale. Blood and saliva samples are collected either at home or at a lab near their home.
Are we like the proverbial frog in water who is slowly being boiled? A very important article on denial and minimization of uncomfortable things including the long term effects of SARS-CoV-2 infection came out in Scientific American. I highly recommend reading it.
H5N1
In Minnesota, heavy rain caused seventeen manure pits from 15 farms in the area to overflow. Flood waters could potentially spread viruses like H5N1 if cattle nearby are infected with H5N1.
H5N1 is an Influenza A virus. Tamiflu (oseltamivir) usually can treat Influenza A viruses, but it turns out that Tamiflu is 16-times less effective against H5N1. So, if someone were infected by H5N1, they probably would need a much higher dose of Tamiflu than is usually prescribed which could potentially have side effects and would require the government to stockpile more medication.
Finland announced this week that they will offer an H5N1 bird flu vaccine to people who work in high risk jobs.
Other news
This week, Eric Topol, Atul Butte, and colleagues put out a “state-of-the-art” review on using artificial intelligence in cardiovascular disease.
The Texas abortion ban from 2021 was found to be associated with an increase in infant deaths in the state. "Abortion restrictions may have negative spillover effects on infant health."
Being exposed to light between 12:30 am and 6 am was found to be associated with an increased risk of developing Type 2 diabetes. “Light exposure at night can disrupt our circadian rhythms, leading to changes in insulin secretion and glucose metabolism,” senior researcher Andrew Phillips.
Anthony Borges was critically injured by gunman Nikolas Cruz in the 2018 Parkland, Florida high school mass shooting. In an unusual civil settlement, Borges now owns the rights to the gunman’s name. The gunman can no longer give any interviews or make money by telling his story without Borges' permission.
56-year-old golfer Frank Bensel Jr. who made back-to-back holes-in-one at the US Senior Open. “No golfer has ever made back-to-back aces in any Tour-sanctioned event on record, according to the PGA Tour Champions.” The odds of making two holes-in-one in a single round are 67 million to one. Congratulations Frank!
Have a good rest of your weekend,
Ruth Ann Crystal MD
P.S. I will be taking off from next week’s newsletter for the 4th of July weekend.













.jpg)