------------------------------------------
Katelyn Jetelina and Hannah Totte, MPH, Mar 03, 2026
Somehow, it’s already March! And there’s a lot unfolding right now at the intersection of society and health. I’ve been especially thinking about Iranians—including my own family—and hoping we can all take a moment to listen and learn. If you’re looking for a place to start, I highly recommend the book All the Shah’s Men.
In the health world, we have flu hanging on, RSV making a surprisingly late appearance, and falling vaccination rates that will cost us more than most people realize. Plus, a reader question worth unpacking: Does the surgeon general actually need an MD?
Here’s what’s going on and, most importantly, what it means for you.
She grew up unvaccinated, she’s an immunologist, and she’s our colleague.
YLE’s own Liz Marnick published an op-ed in the NYT on Friday. I know I’m biased, but it’s a must read. Liz shares her story of growing up unvaccinated, hard conversations with her mother, and going on to study the immune system. And yet, when it came time to vaccinate her own child, she paused:
“In that one exhausted moment, what was loudest in my head was not the science I knew well. It was the stories I had heard growing up.”
Her message: shame doesn’t work. Please read it; it’s a masterclass in approaching this moment with empathy.
Disease “weather” report
This respiratory season just won’t quit. Flu activity is holding steady. One strain (flu B) is rising while another (flu A) is falling, and together they’re canceling each other out. That kind of plateau is unusual; most seasons follow a smoother up-and-down curve. But the timing isn’t surprising. In bad flu years, activity has stayed above epidemic levels well into mid-March.
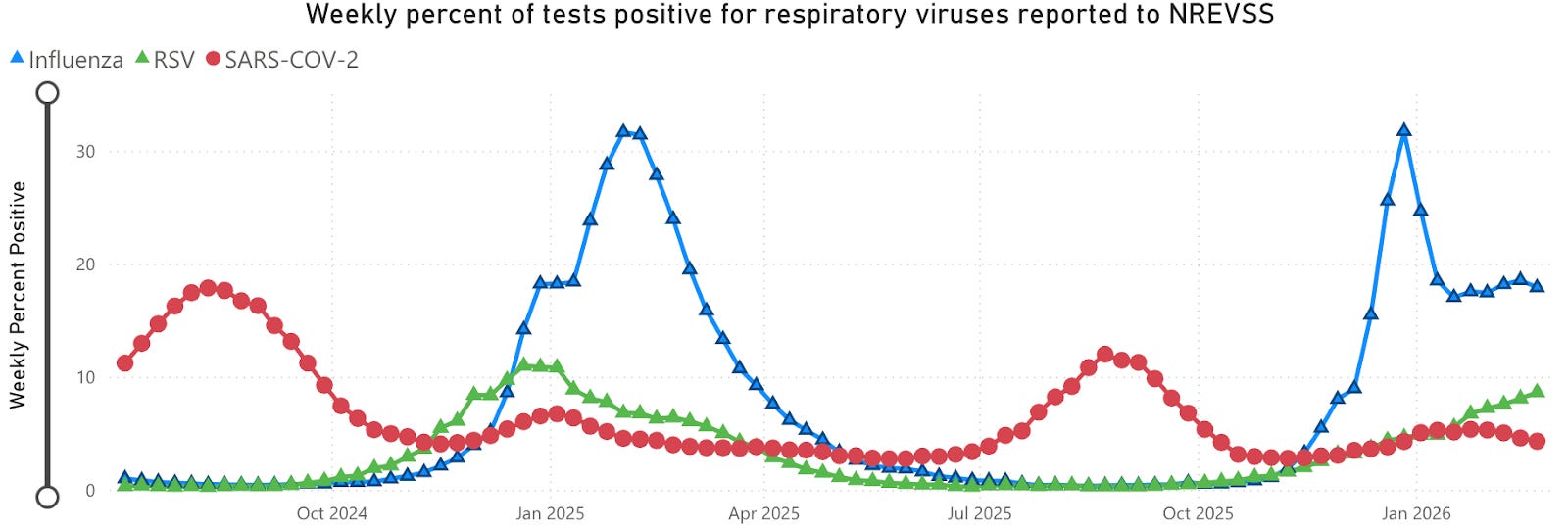
What is unusual is that RSV infections and hospitalizations continue to climb. It’s incredibly late in the season for RSV to show its teeth. Babies are most at risk.
What this means for you: It’s not too late to get your vaccines!
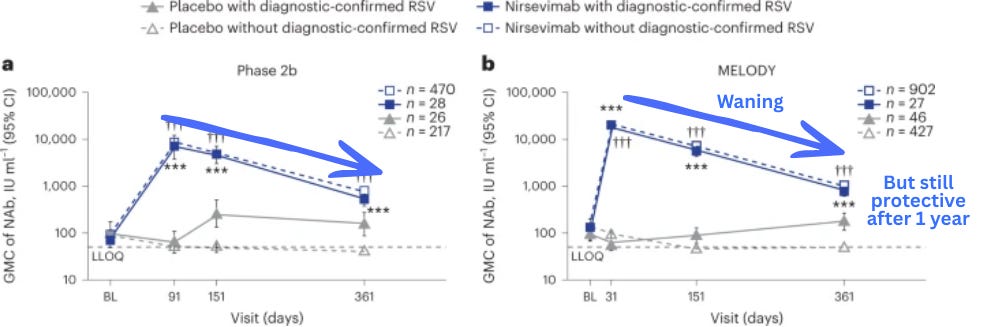
For RSV: If your infant received monoclonal antibodies (like Nirsevimab) this season, they’re likely still protected. Most monoclonal antibodies fade quickly, but the RSV ones were specifically engineered to last longer. Nirsevimab has a half-life of about 70 days—meaning the amount in the body decreases by half roughly every 70 days. Even so, studies show protective levels can persist for more than a year. So even doses given early in the season should still be providing coverage.
AI tools aren’t ready to triage you… yet
People want more control over their own health. Health care is expensive, hard to access, and appointments aren’t always easy to get. There is a lot of promise for AI, and people are already using it for their health: 230 million people ask ChatGPT health questions every week. So if AI tools could reliably help people decide when to seek care, that would be a big deal.
But a new study suggests we’re not there yet.
Researchers published a study last week in Nature Medicine testing ChatGPT Health, a new consumer health AI tool, on a basic but critical task: triage. Given a set of symptoms, could it correctly tell you whether to stay home, schedule a routine appointment, get seen urgently, or go to the ED?
The results were mixed, and concerning at the extremes:
For people who didn’t need a doctor at all, it sent them to one 65% of the time. A waste of time and money.
For routine visits, it correctly recommended seeing a doctor 95% of the time.
For people who needed emergency care, it only recommended the ED about half the time. It handled classic emergencies well, like allergic reactions or stroke, but struggled to recognize how sick someone was about to become, like the early stages of a diabetic complication.
More detailed medical data improved accuracy, but adding irrelevant information confused it. For example, when normal lab results were included alongside a note that a patient was suicidal, ChatGPT got it wrong. That’s obviously deeply concerning.
What this means for you: For straightforward health questions, AI tools can genuinely help and can certainly supplement a visit with a clinician. Add more details for more accuracy, but proceed with caution and certainly do not use it for emergency health issues.
And so it begins: Hep B birth vaccine rates are going off a cliff
One of the biggest open questions right now is how far vaccination rates will fall in the current climate before they level off and begin to climb again. Tracking vaccination rates in the United States is surprisingly difficult because we do not have a single, centralized, easily accessible system like countries such as Denmark do. Instead, data are fragmented across states and systems.
Still, early numbers are starting to come in, and the picture is not encouraging.
A group of researchers analyzed de-identified medical records from 2016–2025 to track hepatitis B vaccination trends. They asked: How far have we drifted from the expected path?
It turns out, quite a lot. For every 100 live births, 10 fewer newborns received the hepatitis B vaccine than models predicted. The decline began in late 2024 and now appears to be accelerating. (Note: The study period ended before RFK Jr. made the unilateral decision to stop recommending the hepatitis B vaccine for all newborns. That means the downward trend will continue.)
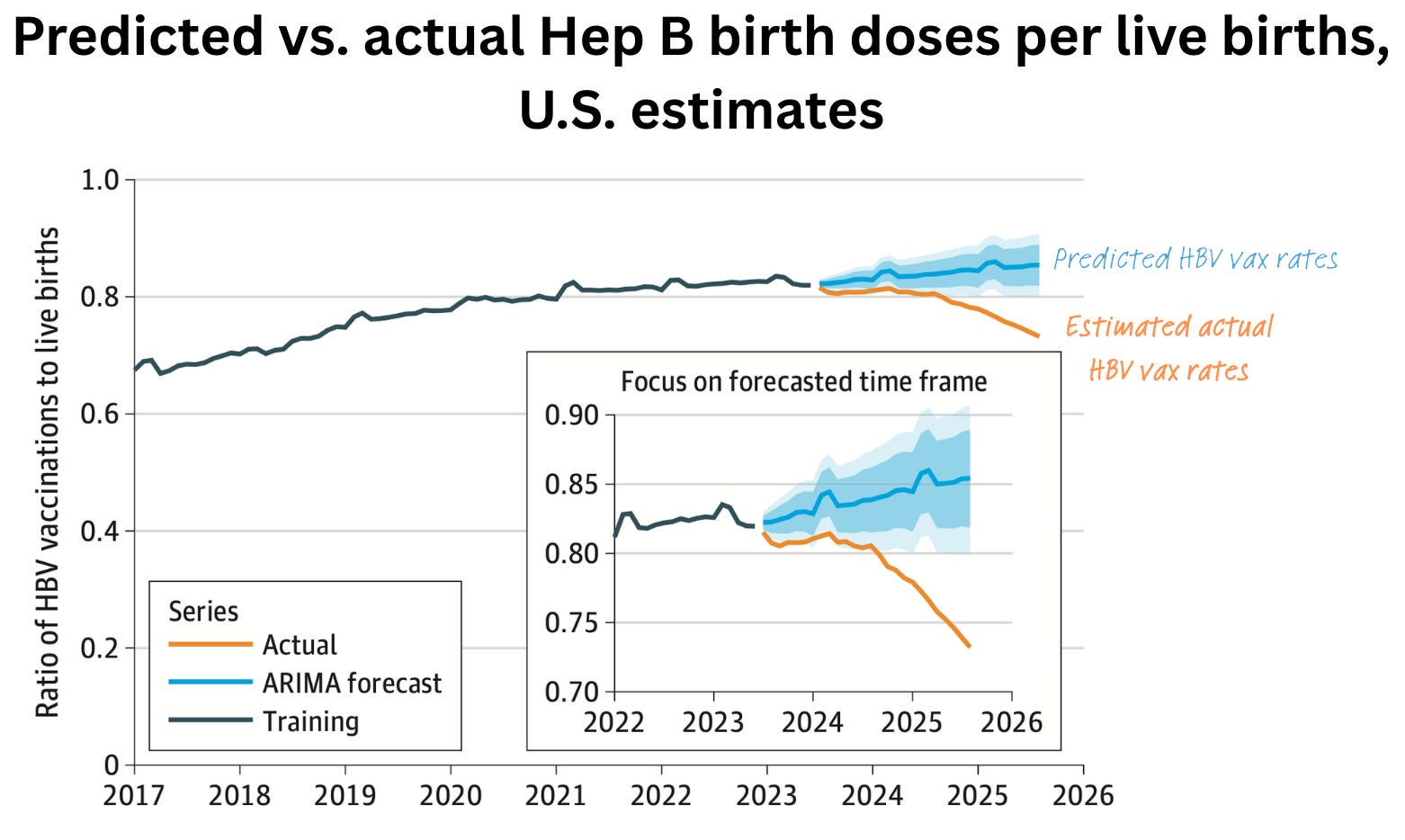
This is unsurprising in a way, but very concerning. I would love to see the findings repeated using other data sources. Unfortunately, this research is brief, and the methods aren’t described in great detail. But clearly, we aren’t going in the right direction in protecting babies’ health and wellness.
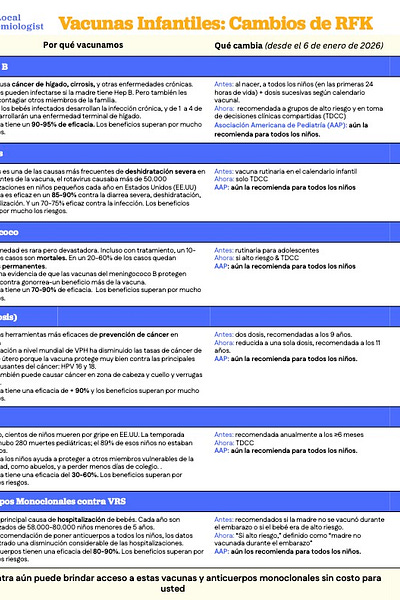
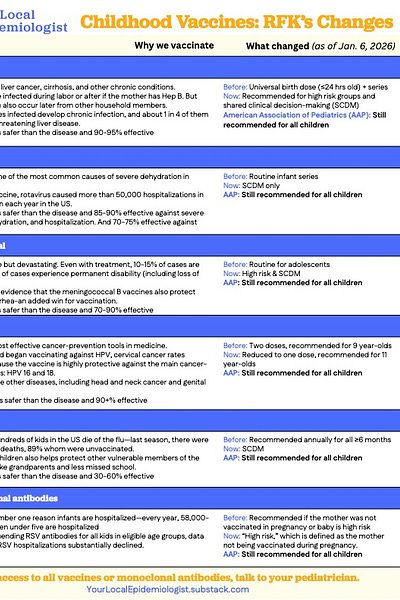
What this means for you: Continue to follow the AAP immunization schedule, which includes the hepatitis B birth dose. If you have questions, talk to your pediatrician.
If you’re navigating Hep B birth dose conversations with parents, what questions about routine immunizations are you getting? Do you believe this trend given what you’re seeing on the ground? Drop in the comments below.
Remember, YLE has this one-pager that includes the recent routine childhood immunization changes and reminders on why we vaccinate for these diseases, like Hepatitis B, in the first place. Feel free to print and distribute!
More measles = more economic cost
Infectious diseases mean people stay home sick and miss out on work, and health care bills are higher. They are also expensive for public health departments to combat. They’re not just a health problem. They’re an economic problem.
Thanks to a Common Health Coalition report, the U.S. now has economic numbers tied to declining MMR vaccination rates.
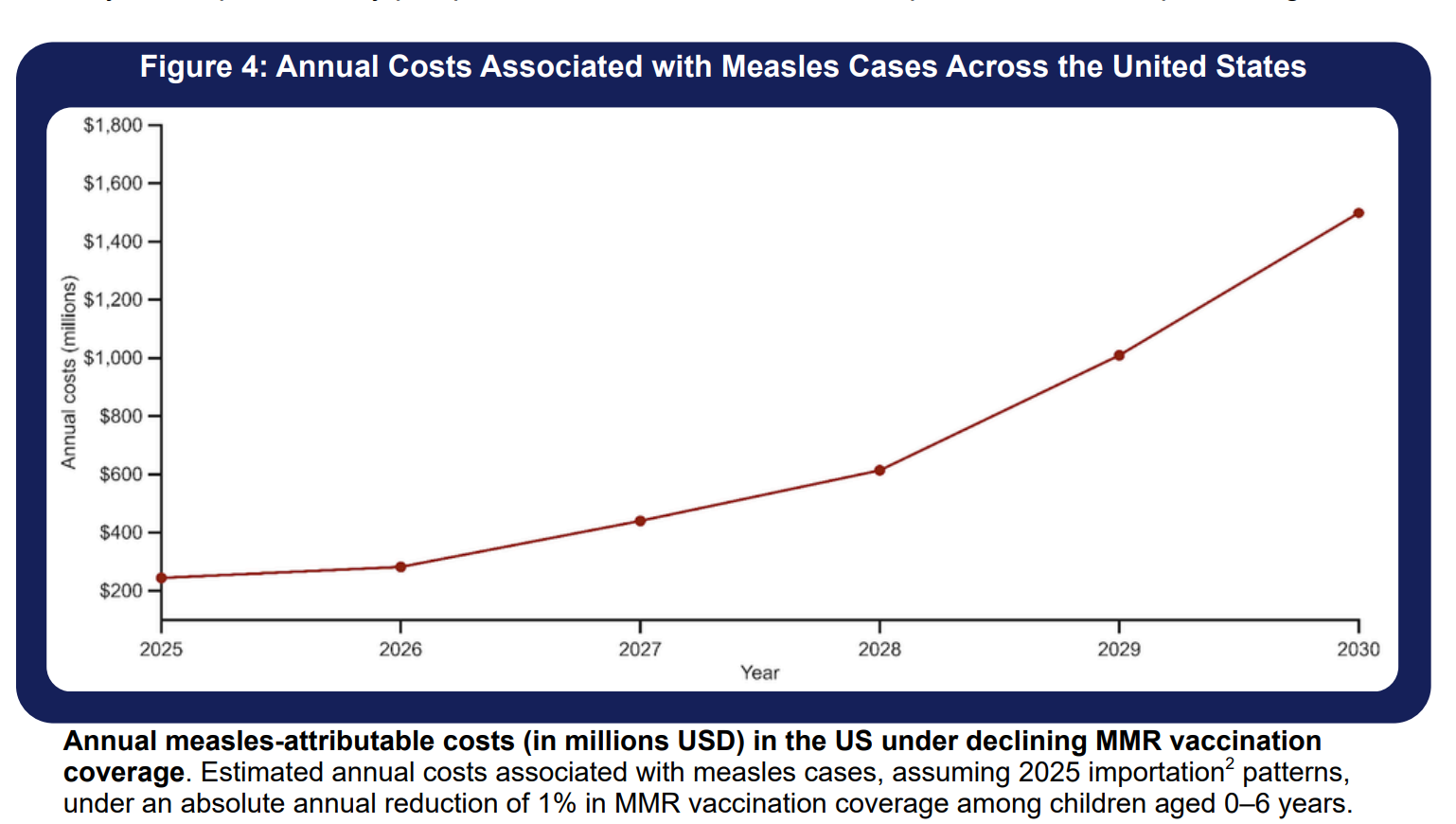
A 1% annual decline in MMR vaccination rates would lead to:
More suffering. Specifically, more than 17,000 measles cases, 4,000 hospitalizations, and 36 preventable deaths each year.
Major economic costs. On average, one measles case costs the U.S. health system $76,000. With the projected number of cases over 5 years, the estimated cost would be $1.5 billion. This breaks down to:
$41 million in medical costs (i.e., medical bills)
$947 million in outbreak responses (e.g., contact tracing, community outreach, surveillance)
$510.4 million in lost productivity and missed work costs
Childhood immunization is as essential to health system stability as it is to community health.
Importantly, this isn’t inevitable. It can be stopped. This report included solutions highlighting that everyone, from health insurers to health departments to clinicians, has a role to play.
What this means for you: As vaccine rates continue to decline, costs will be borne by you, your state, and your health insurance companies. Continue to urge your insurance company to cover routine childhood immunizations at no cost.
For those advocating for immunizations with local, state, or federal decision-makers, be sure to include economic costs. This can be compelling to those who prioritize budgets and resource allocation, since framing immunization as a cost-saving investment (rather than just a health measure) can be persuasive.
Question grab bag
“Serious question: Shouldn’t the surgeon general have a license to practice medicine?”
Short answer: Yes.
Most people know the surgeon general as “America’s doctor,” which is essentially a megaphone for public health. They have delivered landmark messages like those linking smoking to cancer. That role alone demands real expertise and credibility, but I would argue someone with a PhD in public health could do that as easily as an MD.
The lesser-known reason is that the surgeon general commands the Commissioned Corps of the U.S. Public Health Service, a uniformed branch of 6,000 officers deployed into national emergencies, like hurricaines and disease outbreaks. The corps requires its own officers to hold an active, unrestricted medical license and complete residency training. This means that if Casey Means is confirmed as surgeon general (a big if right now), she would be responsible for enforcing standards she doesn’t meet.

In case you missed it
CA YLE Matt’s colon cancer screening PSA.
NY YLE Marisa on the blizzard and police response to mental health crises.
And a measles brief for Christian communicators in an attempt to break echo chambers.
Bottom line
Stay healthy, neighborly, and safe out there.
Love, YLE













.jpg)
No comments:
Post a Comment